Cosponsors



 together with members of the organisation. Credit:UNICEF")
Feature Story
Confronting the link between HIV and gender-based violence in Jamaica
07 November 2019
07 November 2019 07 November 2019Monique McDonald is an HIV peer educator who tells the story of her childhood with unflinching courage. “I was sexually abused by my uncle at the age of 12 and contracted HIV.”
Ms McDonald has written about her experiences in a book called I am now free. It uses her old diary entries to describe the abuse she suffered as a child and her journey to recovery. Today, she supports young women living with HIV, helping them to come to terms with their status and advising them on adhering to treatment. She has also founded the Ashley Fund to help other sexual abuse survivors to continue their education.
She admits that it’s been a long road.
“I was so depressed, I didn’t know who to trust,” she remembers. “How could this happen, and everybody turned their eyes?”
Rushell Gray reflects on her past with a similar mix of sorrow and disbelief.
“As a young girl everybody turned a blind eye and blamed me. I was the AIDS girl walking around in the community. Nobody said, “this man needs to go to jail.” At one point I almost gave up because the stress was too high,” she said.
Ms Gray now works as a Mentor Mom. The Mentor Mom programme enlists young mothers living with HIV to share their experiences and help other young women coping with similar situations. Mentor Moms answer questions and offer reassurance, accompany young women and girls on their health visits and reinforce clinical guidance on the importance of taking medicines regularly.
Both Ms McDonald and Ms Gray are employees and past clients of Eve for Life, a Jamaican nongovernmental organization that helps to prevent new HIV infections and improve the quality of life of women and children living with or affected by HIV. Clients benefit from peer support groups, psychological care and empowerment programmes.
Joy Crawford and Patricia Watson founded Eve for Life 11 years ago. While supporting young women and girls affected by HIV, they quickly learned that there was a clear link between HIV infection, adolescent pregnancy and child sexual abuse. According to Situation analysis of Jamaican children, a 2018 report by the United Nations Children’s Fund (UNICEF), more than one in five (21%) adolescent girls in Jamaica said that they had survived sexual violence.
As a long-standing provider of technical support and capacity-building around sustainability for Eve for Life, UNICEF is keen not only on supporting girls, but addressing the cultural norms that make them vulnerable.
“There is this pervasive idea that adult men should have some level of access to a girl’s body if they are in their life, supporting the family or something like that,” explains Novia Condell, UNICEF Jamaica’s Adolescent Health and Empowerment Specialist. “Of course, the girl has no power to negotiate any protection in a situation where she has been abused or exploited.”
High on UNICEF’s agenda is supporting the community engagement necessary to shift attitudes around child sexual abuse. Eve for Life has spearheaded the “Nuh guh deh” (don’t go there) campaign, which aims to stop sexual abuse. They use complementary strategies—everything from community meetings to music videos—to get the message out.
The UNAIDS country office in Jamaica also provides technical support to Eve for Life and has helped the organization build partnerships for resource mobilization. The UNAIDS Caribbean subregional office is also working with Eve for Life to create safe spaces for young survivors and leaders to raise awareness about the link between gender-based violence and HIV.
There is also a focus on meeting young women’s basic needs, including food, clothes and health care. But beyond these services, work continues to provide teenage girls and young women living with HIV with a deeper level of emotional support and mentorship.
“Jamaica’s Ministry of Health has found a strong partner in Eve for Life—one that is able to focus on resilience and life skills-building. They get the girls’ lives on track so they can improve their lot and the lot of their children,” says Ms Condell.
Focus on
Region/country
Related





Feature Story
Educational show on how to talk with teenagers about health and sexual relations
21 October 2019
21 October 2019 21 October 2019Originally published by UNESCO on 16 October 2019
On 9 October, Po Pravde Govorya, an educational show by UNESCO, UNAIDS and OK.RU, went live on air to discuss how to talk with teenagers about health and sexual relations. The Russian social network Odnoklassniki hosted Po Pravde Govorya, [Telling the Truth], a live talk show co-organized by the UNESCO Institute for Information Technologies in Education (UNESCO IITE) and the UNAIDS Regional Office for Eastern Europe and Central Asia (UNAIDS EECA). Experts and celebrity parents discussed ways of talking with kids and teens about complex issues such as puberty, sexual relationships, personal boundaries, HIV and AIDS, and much more. The two-hour show hosted by TV presenter and journalist Lika Dlugach, received some 1.3 million views and 1,320 likes from OK.RU users.
The talk show guests included film and theater actress Elena Borshcheva, journalist Tatiana Nikonova, family therapist Marina Travkova, obstetrician-gynecologist Tatiana Rumyantseva, Alfiya Maksutova, editor-in-chief of DVOR, a social media page for youth, Vinay Saldanha, UNAIDS Regional Director for Eastern Europe & Central Asia, and Tigran Yepoyan, UNESCO Regional Health Education Advisor.
They used examples from their personal life and professional practice to illustrate how to discuss sensitive issues with kids and teens in an atmosphere of trust and without embarrassment, how to help young people make sense of what happens to their minds and bodies as they reach the challenging period of puberty, and how to educate them, honestly and non-judgmentally, about the basics of health and relationships.
Should we talk with kids and teens about sex and if so, how to do it right?
Marina Travkova, family therapist
We should tell them the truth in a way that is adapted to their age. But I would like really like all parents to understand that they do not need their child to be a certain age or to pick a special time and place for this conversation. Like it or not, you have been communicating with your kids about sex all the time since the moment they were born, because understanding sexuality is not only about technical knowledge of where babies come from. There is a lot more to it, including how your children feel about themselves, their personal boundaries, whether or not they tolerate uncomfortable clothes, how they feel about being hungry, whether they can refuse to kiss a granny who loves them. All of these are integral parts of our sexuality. The hands of the father and mother who hold and caress the baby build the first layer of what will later become his or her sexuality. How they feel about themselves, their body, the world around, their personal boundaries. We’ve been having this conversation with our kids all the time by sending them messages about the way to live their lives, to make choices, to fall in love, and to treat their bodies. When your child approaches you with a concrete question, this is a moment not to be missed – a moment of trust. Parents who feel at a loss or afraid to say the wrong thing should remember that it’s always possible to say, “I don’t really know, to be honest,” and perhaps find and offer your child a good book on the topic. You also need to understand that today, teens live in an incredibly open world, and the average age they are introduced to pornography is 9 to 11. Indeed, many teens today say or write, “How can I explain to my mom that she needs to read something about sex?” This is the way teens take care of their parents.
What questions do teens want answered?
Tatiana Nikonova, journalist
Most of the time, teens seek answers to questions which have little to do with what adults want them to ask about. What are most parents concerned about? Pregnancy, bad company, sexually transmitted diseases. But teenagers are interested in relationships. What to do and say, how to tell a person you love them, how to survive rejection, how to say no, and how to deal with the fact that everyone knows something about you that you’d rather keep private. Very often, teens struggle with the issues of bullying and aggression. What happens on a date and what can happen besides being offered sex – this is also something they’d like to know.
How to be more confident talking with your children?
Marina Travkova, family therapist
I can share two lifehacks with parents of teenagers. The first is to speak honestly about yourself, e.g. about the first time you fell in love, the first time you said no to a boy who was in love with you and how it made you feel – all of this has great value for your child. The second lifehack is to be honest with them about your fears.
Tatiana Nikonova, journalist
Discuss TV serials with them – something is always happening there! Like, unplanned pregnancies, complex diseases, breakups, misunderstandings – these are the most common stories in TV shows and a virtually endless source of topics for discussion.
Is it true that sex education can encourage young people to have sex earlier in life?
Vinay Saldanha, UNAIDS Regional Director for EECA
Numerous studies in different countries have found that not only sexuality education programs do not lead to an earlier or more active onset of sexual life, but have the opposite effect: adolescents tend to have a later sexual debut, fewer partners, a lower incidence of risky behaviors, and they are more responsible about the use of condoms and contraception. Together, this reduces the risks of contracting HIV and other sexually transmitted infections. Of course, such programs must be age-appropriate, evidence-based and, most importantly, they must be timely, i.e. before children become adults, otherwise it will be too late. This is what is said in the International Technical Guidance on Sexuality Education developed by several UN organization led by UNESCO.
Why do we need to talk with children about HIV if most people who get infected are adults?
Vinay Saldanha, UNAIDS Regional Director for EECA
In EECA countries alone, dozens of thousands of children and adolescents live with HIV. Therefore, we cannot say that this disease does not concern children. But it is essential to have a high-quality sexuality education program to make sure that a discussion of these complex issues brings positive outcomes.
What can we do if a kid does not believe that HIV exists, because they have read on the internet that “HIV is a hoax”?
Tatiana Rumyantseva, obstetrician-gynecologist
Give this kid a link to the website of the World Health Organization, to other sites which discuss infections. There are many organizations of people living with HIV who work to help others. You can take the kid to such an organization and let him or her meet people there. This approach might work well with someone who responds to emotions more than to words.
How to talk about HIV and not scare people?
Tatiana Rumyantseva, obstetrician-gynecologist
This information serves as a warning. Speaking about infections, I would say that some of them cannot be cured but require lifelong treatment. It makes good sense to plant a grain of concern for their future in young people’s minds. We usually spell out the dangers which we want to protect children from, and the same should apply to sex.
What source of information would a teenager trust the most?
Elena Borshcheva, actress
Bloggers. All teens are watching bloggers. Good educational programs for teens on TV are lacking, so young people learn a lot from bloggers. It makes sense to share essential information through their idols.
Recently, I came across a book and read it before giving it to my daughter. The author is American, and some realities are different from ours, but the concept of personal boundaries in relationships not only between a boy and a girl but also between friends is very well explained. And I thought, “Where was this book when I was a child?” It explains, plain and simple, how to act in certain situations, how to check what’s right, and what to say.
We all want relationships in the first place, warm relationships in which we need and love each other, and sex is part of such relationships. But many people – especially young people — do not quite understand why sex is special and whether a girl can refuse a guy, although it is her right. They need to learn how to tell real love from being taken advantage of in a relationship.
Can websites help parents in educating their children, and how can we teach children to safely navigate the diverse resources?
Tigran Yepoyan, UNESCO Regional Health Education Advisor
Absolutely yes. There is an increasing number of such resources available for parents and for teenagers. As far as teenagers are concerned, media literacy is the key, and UNESCO has been working to help countries educate teachers about media literacy, so that they may teach their students. Here are some basic lifehacks: it is essential to help children develop an ability to critically assess and analyze information, never take it for granted but double-check and look at the source of information: who created the website, who are the authors of posted materials, whether they provide links to primary sources and refer to relevant experts and research findings; ask yourself whether the main purpose of the website is to provide objective information or to impose a particular behavior pattern or lifestyle, manipulate the reader, or sell a product or service.
About DVOR, an online community for teens
Alfiya Maksutova, DVOR editor-in-chief
We created DVOR with support from UNESCO to talk with teens about reproductive health. Most of our readers are under 21.
We cover several broad topics. The first is physiology: we discuss a variety of things related to one’s body and health, e.g. how the brain works or myths about penis length. The second is mental health: e.g. what is depression, how to deal with bullying, and how to survive rejection And finally, we discuss sex and everything related to sex.
The more something is taboo, the harder it is to discuss. But we always emphasize that there is nothing shameful about this discussion and we never try to hide behind academic terminology or euphemisms. Our goal is to create a safe and comfortable space for a well-informed discussion of this topic with teenagers. All our posts on the topic are based on recent research, and each text is reviewed by a relevant expert. And we also dilute serious content with comics and entertainment to create an atmosphere of trusting and relaxed communication. Seems like it works: every week, we receive warm and positive feedback from subscribers.
What are some of the approaches used by DVOR in discussing sensitive issues that teens’ parents can adopt?
Parents might find it super useful to look at our page if they plan to discuss such things with their teens. Let’s say I am a parent who wants to talk to their child about watching porn or using contraception. What do I need to know before I bring it up? I need hard facts, statistics, and an idea of how such things work. Because direct advice like “don’t watch porn for 8 hours a day” or “protect yourself if you have sex” aren’t nearly as effective as a fact-based explanation of how people become addicted to porn and why being protected is a good idea. And then I’ll let my child draw their own conclusions. All information that I may need for such conversations can be found on our page, with links to sources and references. Plus, everything is written in a language that teens can relate to and feel comfortable with, without judgment, vulgarity or euphemisms.
Po Pravde Govorya was broadcast live on OK.RU/TEST, an online community created with support from the UNAIDS Regional Office for EECA and UNESCO IITE.
Follow new show announcements, participate in surveys and competitions, and learn new things at OK.RU/TEST
Region/country
Related
 Three Years On: From crisis to prospective recovery
Three Years On: From crisis to prospective recovery
20 February 2025



Feature Story
Empowering young Brazilians to talk to their peers about HIV
11 October 2019
11 October 2019 11 October 2019New HIV infections in Brazil increased by more than 20% between 2010 and 2018, so it’s crucial that young Brazilians start talking about HIV and learn how to protect themselves. That’s the aim of a project led by the United Nations Children’s Fund (UNICEF).
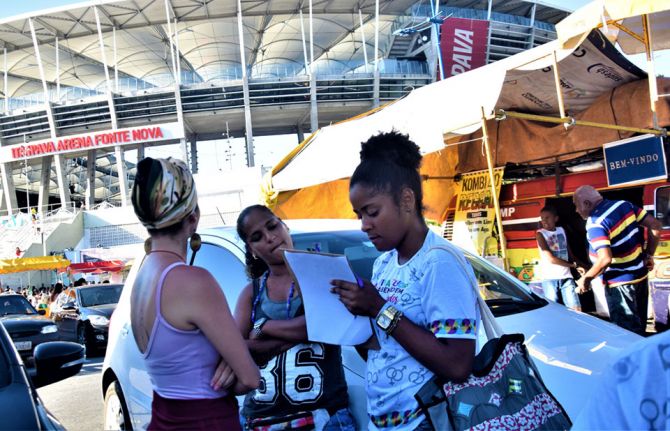
Swiping through one of his social media accounts, Jonas da Silva checks out the latest parties and public events in Salvador. He is also chatting online with other young people. They talk about sex, how and if they use condoms with their partners, what they know about HIV prevention and if they have been tested for HIV.
“What’s cool about the project is that we have young people talking to young people. We use our language and slang to address HIV,” he says. “This connection is vital. We can see they trust us, and this is when we know we have touched them with the information they need.”
He and another 30 young people have been trained to work as volunteers in the Viva Melhor Sabendo Jovem (VMSJ) Salvador project. Their goal is to raise awareness among other young people about the importance of HIV testing and prevention. For that, they need to be where their peers are—online and on the street.
The project follows the calendar of traditional street parties and festivals, especially those that attract a large concentration of young people. It also responds to specific demands from key populations by mapping public gatherings where young lesbian, gay, bisexual, transgender and intersex people hang out. With a colourful small truck—the Test Truck—Mr da Silva and his co-volunteers can provide privacy for people who want HIV counselling and testing.
Since the project launched in August 2018, more than 1000 young people aged between 16 and 29 years have been tested for HIV in around 30 outings for the truck. As part of a strategy to promote testing among adolescents and young people, the volunteers also facilitate workshops on HIV and other sexually transmitted infections and host talks about sexuality and sexual health in schools. These events reached more than 400 students in the first six months of the project.
“The VMSJ Salvador peer education methodology makes it possible to engage more young people in these activities. It also helps them to become aware of the importance of HIV prevention and care,” said Cristina Albuquerque, Chief of Health and HIV/AIDS for UNICEF in Brazil. “Young people who get tested during our activities congratulate the initiative and complain that they have very few of these opportunities around town.”
In 2018, according to Ministry of Health estimates, young people aged between 15 and 24 years represented almost 15% of all new HIV diagnoses in Salvador.
“For us, too, the volunteers, this experience is important because we also start to take better care of ourselves, to apply these prevention methods to our lives and to pass the message on to those around us, to our friends and family,” said Mr da Silva.
The project is implemented in partnership with GAPA Bahia―one of the oldest nongovernmental organizations dealing with HIV issues in the country―and counts on the support of the UNAIDS office in Brazil. The young volunteers all went through a rigorous selection process before undergoing a training programme that included topics such as human rights, counselling and information on HIV and other sexually transmitted infections. They were also trained on community-based programmes, the functioning of the public health system and HIV services available in Salvador. The initiative includes a continuous training strategy on related topics.
“One of the most important things I have learned is that we have to respect each other’s choices and that we are here only to assist with information and inputs that we consider most appropriate to that person’s history and behaviour”, said Islan Barbosa, another of the volunteers.
“The project represents an important response to HIV testing demands in the city, especially among key populations, who very often avoid using public health facilities for that purpose. We are taking HIV testing to where these people are,” said Ms Albuquerque.
Focus on
Region/country




Feature Story
Preparedness, proactiveness and speed are key to tackling humanitarian emergencies
15 August 2019
15 August 2019 15 August 2019When Cyclone Idai hit Mozambique and the eastern part of Zimbabwe in mid-March, it couldn’t have come at a worse time. A month earlier, Zimbabwe had issued an emergency appeal for some 5.3 million people affected by an ongoing economic crisis, and limited rainfall had ruined crops. The sudden pounding rain and wind threw everything into chaos. Three hundred people died, hundreds disappeared and 40 000 lost their homes. Food insecurity plus a lack of basic services, including health care, skyrocketed in the hardest hit province of Manicaland.
For Mumtaz Mia, the UNAIDS Acting Country Director in Zimbabwe at the time, the most pressing issue was to ensure that people living with HIV, including pregnant women enrolled in prevention of mother-to-child transmission of HIV programmes, could access HIV treatment.
“In Zimbabwe, where emergencies are not a new phenomenon, people living with HIV were left stranded when their medicine got washed away,” she said.
For her, preparedness is key. “For the AIDS response, we must anticipate any disruptions to services that emergencies bring.”
Born in Malawi, Ms Mia has dealt with droughts and floods throughout eastern and southern Africa. She also spent some time in Kenya dealing with post-election conflict and worked five years in South Sudan for UNAIDS before her stint in Zimbabwe.
She recounted that the UNAIDS country office met with the government, civil society, donors and other key stakeholders to discuss immediate action. Quickly, they made sure that HIV-specific needs were integrated in the emergency response. That meant coordinating, with UNAIDS Cosponsors, the Ministry of Health and Child Care and the National AIDS Council, to ensure the distribution of antiretroviral therapy and condoms, food support for people living with HIV and safe deliveries for pregnant women. They also set up assessments to address additional health and HIV needs following the disaster.
Almost 150 000 people living with HIV were in the cyclone-affected districts, and about 83% of them were accessing antiretroviral therapy. Most of them experienced a disruption of treatment during the crisis.
“Without a clear plan and instructions on action that needs to be taken in an emergency, precious days and weeks can be wasted trying to figure out what to do,” Ms Mia said.
She also believes that interagency contingency plans with specific tasks assigned to each agency to be taken in the event of an emergency would help action to be taken more quickly. “Using simple and clear guidance on the actions required by UNAIDS in emergency situations and the impact they can have on HIV are critical to guide country offices and managers,” she said, adding that “It’s important to earmark financial resources so that you can access and use the money right away.”
She practises yoga to help cope in times of stress and praises her supportive husband. “We try to have a semblance of a normal life at home during chaotic times,” she said, although she admits that often it is not easy. Throughout, she focuses on the people that needed her help. “I leave my door open, I listen to their stories and that gives me perspective to forge ahead.” That’s why she reiterated that in time of need, you cannot let people down. “Speed is of the essence.”
The UNAIDS Country Director for the Bolivarian Republic of Venezuela, Regina Lopez de Khalek, agrees. “In a humanitarian emergency, you have to act really quick in order to save lives, which means reinventing your everyday tasks to focus solely on the crisis,” she said.
In her case, she is dealing with the impact on people living or affected with HIV, of a political and economic crisis that affects more than 80% of the population. Inflation in the Bolivarian Republic of Venezuela has exploded, making basic food items beyond reach. Shortages have plagued the country, and medicine is no exception. Since May 2019, the country has recognized that there are some “humanitarian needs”, facilitating the delivery of medicine and rapid HIV and syphilis tests. With the help of international nongovernmental organizations, almost 60 tonnes of life-saving medicine have been delivered to the country. UNAIDS also worked for the country to receive emergency funds from partner organisations.
More recently, UNAIDS, the United Nations Population Fund and the Office of the United Nations High Commissioner for Refugees have jointly focused efforts to help people affected by stigma, discrimination and sexual violence. This included distributing post-exposure preventive kits, an emergency medical response for people exposed to HIV, to health services and introducing HIV tests to maternity units, as well as supporting civil society.
For Ms Lopez de Khalek, working jointly with other United Nations agencies and partners on the ground makes all the difference. “Not only does working hand in hand make sense, but it allows the AIDS response to stay relevant in a humanitarian situation,” she explained.
She recommends following the Inter-Agency Standing Committee HIV Task Force in Humanitarian Settings guidelines, but not to overlook the local and national context. “Know and understand the situation of the country you are in,” she said, “because although emergencies may seem equal, each crisis takes on the particularities of the country in which they occur.” And be proactive. “Act accordingly in advance, so that you are not just reacting,” she said. In her mind, it’s key to set up relationships, collaborate and engage with others and build a comprehensive response so that in the event of an emergency you and the people you are there to help are not left behind.
Simone Salem echoes that sentiment. “The key asset that helped me to respond to emergencies has always been the number of contacts I had across the countries as well as good relations with key people who were able to help,” the UNAIDS Community Mobilization Adviser in the Middle East and North Africa region said.
She added that when you start acting and giving concrete help, people will trust you and seek your support.
Ms Salem describes her work in Iraq, Libya and the Syrian Arab Republic as life-changing. “With each person I help, I realize the importance of my job and how crucial it is to always be alert to people’s needs,” the Egyptian said.
Recently, she helped people migrating or fleeing their homes to access HIV treatment and counselling. With the help of activists and regional networks, she supported the evacuation of lesbian, gay, bisexual and transgender (LGBT) people who had been targets of violence.
In times of crisis, she admires the solidarity that sprouts up at all levels. For example, Tunisians recently offered to give surplus HIV treatment to Libyans. The same occurred at the height of the Syrian conflict, with Lebanese people donating medicine.
Over time, she has become a much better decision-maker. Her secret? “Listen to what is said and also what is not being said, when analysing complex situations,” Ms Salem explained.
In her mind, it’s not a question of gender but of personality, although she said that women and vulnerable people she worked with came to her because they felt that she may be more supportive. The only regret she has is when she cannot help someone. “That’s very hard.”
Using her heart is how she explained she listened to people. When young LGBT people came to her saying that her comforting words had given them hope, she was touched.
“That was so precious to me and really keeps me going," Ms Salem said. “I push and push so that people are treated fairly and with compassion.”


Feature Story
Empowering women living with HIV in Djibouti to live dignified lives
25 July 2019
25 July 2019 25 July 2019Zarah Ali (not her real name) remembers how things changed for the better. “In 2014, I received a loan of 40 000 Djiboutian francs (US$ 250) that I used to develop and improve my garment business. I was also trained in business entrepreneurship, including marketing and customer satisfaction. I import clothes from Dubai and Somaliland and earn a decent income that helps me support my 25-year-old son, my 16-year-old daughter in secondary school and my three-year-old adopted son. I am able to pay for my rent, electricity and water and have decent meals.”
Ms Ali’s loan came from an income-generation programme established by the World Food Programme in collaboration with the United Nations Development Programme, UNAIDS and the national network of people living with HIV in Djibouti (RNDP+). The programme supports the long-term empowerment of, and provides regular incomes to, women living with HIV in Djibouti City. It helps them to achieve financial security and have access to food and improves their access to health-care services. Income-generating activities such as those supported by the programme have a powerful potential to help people living with HIV adhere to antiretroviral therapy and optimize health outcomes.
The loans, ranging from US$ 141 to US$ 438 per person, are for starting or building retail businesses. The beneficiaries, who are selected from among two networks of people living with HIV affiliated to RNDP+ (ARREY and Oui à la Vie – Yes to Life), also receive training on how to run their business. Government support in the form of favourable policies and legislation has been vital to the success of the programme.
Dekah Mohammed (not her real name) now lives a fulfilling life after receiving help from the income-generation programme. Ms Mohammed, who lost her husband to AIDS, lives with six children. After she lost her job in the hospitality sector owing to her deteriorating health and to stigma and discrimination, she started her own clothing business and received a loan of 50 000 Djiboutian francs (US$ 313) to expand her business. The loan was repaid within 10 months. Her business has since expanded into furniture and electronics and she has recruited an employee. “I am no longer a desperate woman. I make enough to take care of my family and dependants,” she said.
The programme has improved the quality of life of many Djiboutian women, allowing them to regain dignity and ensure their financial security. It empowers women and girls to protect themselves from HIV, make decisions about their health, live free from violence and be financially independent.
Building on the belief that empowering women living with HIV and their households to be financially independent strengthens adherence to treatment and leads to more fulfilling and dignified lives, the programme contributes to the World Food Programme’s broader strategic contribution towards ending AIDS as a public health threat by 2030.
Region/country
Related



Feature Story
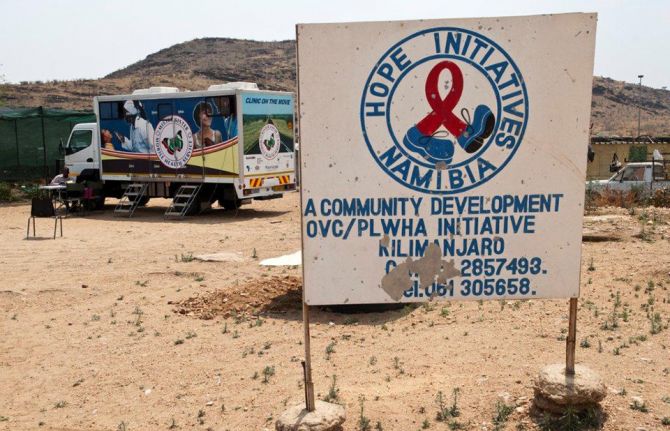
“The staff at the clinic are very friendly. I am an old client so they all know me very well”
02 July 2019
02 July 2019 02 July 2019This story was first published by UNFPA
Windhoek, NAMIBIA - Sometimes it is best to go where everyone does not know your name, but where you feel welcome just the same. It is that way for many sex workers and men who have sex with men (MSM) in Namibia, who bear the brunt of criticism, repulsion and stigmatism in almost all aspects of their daily lives.
As a result, these men and women shy away from accessing essential health services, such as HIV testing/treatment, prophylaxis (PrEP), condoms, lubricants and contraceptives.
According to the first ever integrated bio-behavioral surveillance study (IBBSS) 2014, among MSM in Namibia, HIV prevalence among MSM was estimated to be 10.2 per cent in Keetmanshoop, 7.1 per cent in Oshakati, 10.1 per cent in Swakopmund/Walvis Bay, and 20.9 per cent in Windhoek the capital city.
The estimated HIV prevalence estimated among MSM in Oshakati and Swakopmund/Walvis Bay approximated that of the general population of adult males in the surrounding Oshana and Erongo regions, as measured by the Namibia Demographic and Health Survey, 2013.
HIV prevalence among MSM in Keetmanshoop was slightly lower than that of the general population of adult males in Karas Region, while HIV prevalence among MSM in Windhoek was nearly twice as high as HIV prevalence among adult males of the general population in Khomas Region.
Non-judgemental care
In 2018, the Namibia Planned Parenthood Association (NAPPA) with support from United Nations Population Fund (UNFPA) Namibia convened several advocacy meetings with key partners aimed at establishing a drop in centre at the Out Right Namibia offices.
Out Right Namibia is a Namibian organisation working with the lesbian, gay, bisexual, transgender and intersex (LGBTI) community aimed at advancing the rights, interests and expectations of the LGBTI community in Namibia.
Both the drop in centre and NAPPA Okuryangava clinic had flexible working hours to allow key population to access sexual and reproductive health (SRH) and HIV services at their convenient times, it also involved opening the clinic on Saturdays to allow key population to access services without fear of stigma and discrimination.
All service providers and staff at the drop in centre and clinic were trained and sensitised on the importance of quality, non-judgemental service provision to key population. The staff at Outright Namibia were also mobilised to build awareness and information about the services being provided at the drop in centre and clinic.
Pleasant experience
“I have had a very pleasant experience visiting NAPPA. As a sex worker, it is important that I feel comfortable and go to clinics where I’m free of judgement. NAPPA has opened their doors for me and I feel at home. There are no complications here as the services are free and I prefer this clinic over local hospitals,” said sex worker, Martha Keto (not her real name).
Keto, 30, has been a sex worker for almost 12 years and has been receiving PrEP treatment at the clinic since October 2017. ”I come regularly for my tests and for PrEP treatment which keeps me protected from contracting HIV. The testing I receive here not only keeps me updated on my HIV or STI status, but it keeps up with my overall health. I am informed about a lot of health information including my liver and the nurses are even able to tell if my alcohol consumption is too high,” she said.
“The staff at the clinic are very friendly. I am an old client so they all know me very well. I would recommend NAPPA services to my colleagues who are also workers. Their doors are always open for us, even during weekends we are able to come in if needed. There is a large number of sex workers in Namibia and I hope the services provided by NAPPA could be exposed so that more sex workers will be informed of the free services that are offered here,” she said.
Keto’s sentiments are shared by Cinton Nati and Gideon Markus, (not their real names) who are both homosexual males receiving services at the NAPPA clinic.
“If it had not been for the friendly staff at the NAPPA clinic and their constant support and encouragement, I would have not visited the clinic as recommended by the nurse,” said Nati. He said this made it easy for him to develop a personal relationship with the clinic’s staff because they were very encouraging and as a result, he was able to see major improvements not only in his health but also his confidence.
Prior to visiting NAPPA, Nati experienced emotional and mental difficulties associated with being newly diagnosed with HIV. As a result, he would often miss his appointments as he found it difficult to accept the reality of being newly diagnosed with HIV.
“Since the very first time my partner and I went to the NAPPA clinics, both at Out Right Namibia and at Okuryangava, we have been treated very well and the staff have gone out of their way to make us feel safe. I have had counselling sessions to make sure that I am doing alright and also checkups to make sure the medication is not having any side effects on my body and that I remain healthy. The staff at the clinics have also regularly checked that we understand how to look after ourselves and that we practice sound sexual health guidelines,” said Markus.
“Each time we visited the clinic at Okuryangava, Sister Fungai Bhera (Senior Registered Nurse) would first make time to chat to us about how we have been. This might sound like a small thing to others, but to me, it means the world as I know she cares about us and that I am taken care of and in safe hands,” said Van Den Berg.
He alluded: “LGBTI community in Namibia has never had proper support from our country’s leaders and as a result, there is still a lot of LGBTI people that get discriminated against and live in fear of their communities as we do not enjoy the same legal rights. Hence we live very secretive lives, sometimes even double lives. I think it is these secret lives that make it easy for LGBTI people in Namibia to land in situations where they are highly vulnerable to getting infected with HIV and other sexually transmitted infections.”
More KPs accessing services
In 2018, a total of 523 KPs were reached with sexual and reproductive health services at the two sites. This included 233 sex workers, 188 men who have sex with men 70 truck drivers and 32 women who have sex with women. A total of ten outreach events were held targeting KPs at various hotspots in Windhoek.
The comprehensive service package provided at the two sites included: HIV testing and counselling, those who tested positive were immediately enrolled for treatment; PrEP services, those who tested negative were also counselled and informed about PrEP services and those who agreed were enrolled on PrEP; family planning services including condoms; sexually transmitted infections (STIs) screening and treatment; and information education related to SRH, HIV and gender-based violence.
Region/country
Related
 clinic in Mombasa, Kenya. Credit: WHO")
Feature Story
Pushing for harm reduction success in Burundi
25 June 2019
25 June 2019 25 June 2019This story was first published by WHO
Getting life-saving harm reduction services to people who use drugs in Burundi was the aim of a recent learning trip to Kenya supported by the World Health Organization (WHO). This saw a team of Burundian physicians and health advocates travel to Mombasa County, Kenya, to learn about good practice from one of the pioneers of harm reduction on the African continent.
Led by Burundian non-profit, Jeunesse au Clair Medical (JCM), the team will push for a comprehensive package of harm reduction interventions in Burundi. Like many other countries in Africa, injecting drug use is not often acknowledged, and a public health response therefore not implemented.
Drug use is widely criminalised and stigmatised and its complexities misunderstood. WHO defines harm reduction as an evidence-based public health response that includes the provision of needle and syringe programmes (NSP), opioid substitution therapy (OST) and access to testing and treatment of HIV, tuberculosis (TB) and viral hepatitis B and C.
Keen to gain insight into the Kenyan experience and inform the development of a programme in Burundi, the Burundian team of doctors, a counsellor and a national coordinator of a network of people who used drugs, visited the Reach Out Center Trust in Mombasa. They observed the delivery of OST programmes and learnt about advocacy with local influencers – in an excellent example of south-to-south learning.
Kenya’s response to minimising the adverse effects of drug use, although not without its own challenges, has succeeded largely through grassroots advocacy and on-boarding key influencers – making it easier for harm reduction to be accepted. This multi-level approach includes collaboration between government and civil society, involving both law enforcement and networks of people who use drugs.
At a visit to the Mombasa Inspectorate in charge of drug-related offences, the team learnt first-hand from the Chief Inspector the importance of police engagement, highlighting the negative impact drug use can have on young lives and the need for strategies that work. Today, some 100 police officers in Mombasa are trained on harm reduction with their work focusing on supporting, not punishing.
In addition to police buy-in, identifying other key influencers such as spiritual and village leaders, other government officials, and people who use drugs themselves, can ensure that harm reduction programmes are effective and sustainable.
Advocacy wasn’t the only thing on the agenda, the team from Burundi also saw in practice how the Kenyan clinics functioned, how methadone is dispensed, they spoke with peer educators and outreach officers, and were trained on data collection for programme monitoring. An important learning if they want to show evidence to get government and donors on their side.
While Kenya is several years ahead in its harm reduction journey, with local input, their learnings can be adapted to other contexts.
“The burden caused by drugs requires interventions at grassroots and education must be provided by trained people to avoid misinformation,” said Dr Egide Haragirimana, clinical officer at JCM.
JCM are putting into action their learnings and will next be involving networks of people who use drugs to better understand what their needs are, to inform future harm reduction initiatives.
Region/country
Related
 Impact of the pause of US foreign assistance in Côte d'Ivoire
Impact of the pause of US foreign assistance in Côte d'Ivoire
19 February 2025
Press Release
UNAIDS and UNDP call on 48* countries and territories to remove all HIV-related travel restrictions
27 June 2019 27 June 2019New data show that in 2019 around 48* countries and territories still have restrictions that include mandatory HIV testing and disclosure as part of requirements for entry, residence, work and/or study permits
GENEVA, 27 June 2019—UNAIDS and the United Nations Development Programme (UNDP) are urging countries to keep the promises made in the 2016 United Nations Political Declaration on Ending AIDS to remove all forms of HIV-related travel restrictions. Travel restrictions based on real or perceived HIV status are discriminatory, prevent people from accessing HIV services and propagate stigma and discrimination. Since 2015, four countries have taken steps to lift their HIV-related travel restrictions—Belarus, Lithuania, the Republic of Korea and Uzbekistan.
“Travel restrictions on the basis of HIV status violate human rights and are not effective in achieving the public health goal of preventing HIV transmission,” said Gunilla Carlsson, UNAIDS Executive Director, a.i. “UNAIDS calls on all countries that still have HIV-related travel restrictions to remove them.”
“HIV-related travel restrictions fuel exclusion and intolerance by fostering the dangerous and false idea that people on the move spread disease,” said Mandeep Dhaliwal, Director of UNDP’s HIV, Health and Development Group. “The 2018 Supplement of the Global Commission on HIV and the Law was unequivocal in its findings that these policies are counterproductive to effective AIDS responses.”
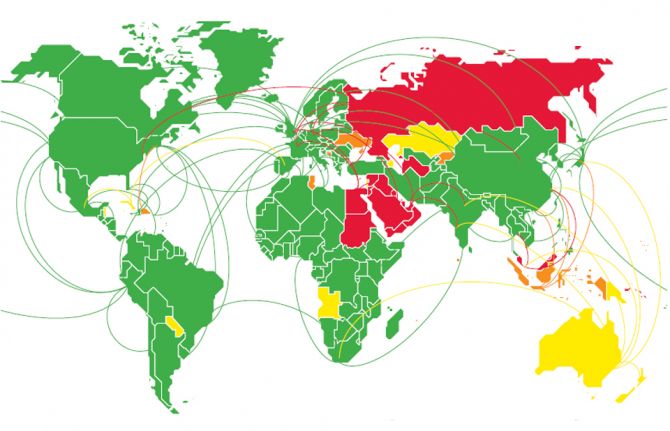
Out of the 48 countries and territories that maintain restrictions, at least 30 still impose bans on entry or stay and residence based on HIV status and 19 deport non-nationals on the grounds of their HIV status. Other countries and territories may require an HIV test or diagnosis as a requirement for a study, work or entry visa. The majority of countries that retain travel restrictions are in the Middle East and North Africa, but many countries in Asia and the Pacific and eastern Europe and central Asia also impose restrictions.
“HIV-related travel restrictions violate human rights and stimulate stigma and discrimination. They do not decrease the transmission of HIV and are based on moralistic notions of people living with HIV and key populations. It is truly incomprehensible that HIV-related entry and residency restrictions still exist,” said Rico Gustav, Executive Director of the Global Network of People Living with HIV.
The Human Rights Council, meeting in Geneva, Switzerland, this week for its 41st session, has consistently drawn the attention of the international community to, and raised awareness on, the importance of promoting human rights in the response to HIV, most recently in its 5 July 2018 resolution on human rights in the context of HIV.
“Policies requiring compulsory tests for HIV to impose travel restrictions are not based on scientific evidence, are harmful to the enjoyment of human rights and perpetuate discrimination and stigma,” said Dainius Pūras, Special Rapporteur on the right of everyone to the enjoyment of the highest attainable standard of health. “They are a direct barrier to accessing health care and therefore ineffective in terms of public health. I call on states to abolish discriminatory policies that require mandatory testing and impose travel restrictions based on HIV status.”
The new data compiled by UNAIDS include for the first time an analysis of the kinds of travel restrictions imposed by countries and territories and include cases in which people are forced to take a test to renew a residency permit. The data were validated with Member States through their permanent missions to the United Nations.
UNAIDS and UNDP, as the convenor of the Joint Programme’s work on human rights, stigma and discrimination, are continuing to work with partners, governments and civil society organizations to change all laws that restrict travel based on HIV status as part of the Global Partnership for Action to Eliminate all Forms of HIV-Related Stigma and Discrimination. This is a partnership of United Nations Member States, United Nations entities, civil society and the private and academic sectors for catalysing efforts in countries to implement and scale up programmes and improve shared responsibility and accountability for ending HIV-related stigma and discrimination.
*The 48 countries and territories that still have some form of HIV related travel restriction are: Angola, Aruba, Australia, Azerbaijan, Bahrain, Belize, Bosnia and Herzegovina, Brunei Darussalam, Cayman Islands, Cook Islands, Cuba, Dominican Republic, Egypt, Indonesia, Iraq, Israel, Jordan, Kazakhstan, Kuwait, Kyrgyzstan, Lebanon, Malaysia, Maldives, Marshall Islands, Mauritius, New Zealand, Oman, Palau, Papua New Guinea, Paraguay, Qatar, Russian Federation, Saint Kitts and Nevis, Samoa, Saudi Arabia, Saint Vincent and the Grenadines, Singapore, Solomon Islands, Sudan, Syrian Arab Republic, Tonga, Tunisia, Turkmenistan, Turks and Caicos, Tuvalu, Ukraine, United Arab Emirates and Yemen.
UNAIDS
The Joint United Nations Programme on HIV/AIDS (UNAIDS) leads and inspires the world to achieve its shared vision of zero new HIV infections, zero discrimination and zero AIDS-related deaths. UNAIDS unites the efforts of 11 UN organizations—UNHCR, UNICEF, WFP, UNDP, UNFPA, UNODC, UN Women, ILO, UNESCO, WHO and the World Bank—and works closely with global and national partners towards ending the AIDS epidemic by 2030 as part of the Sustainable Development Goals. Learn more at unaids.org and connect with us on Facebook, Twitter, Instagram and YouTube.
Contact
UNAIDS GenevaAnne-Claire Guichard
tel. +41 22 791 2321
guicharda@unaids.org
UNAIDS Media
tel. +41 22 791 42 37
communications@unaids.org
Press centre
Download the printable version (PDF)

Feature Story
Positive health, education and gender equality outcomes for Myanmar youth
14 June 2019
14 June 2019 14 June 2019This story was first published by UNESCO
Young people in Myanmar make up more than half of the national population, with 5-14-year-olds making up the largest group. This youthful population brings incredible potential for sustaining Myanmar’s recent development momentum, but only if investments are made to address the challenges that prevent them from making informed decisions about their health and well-being.
Research shows that young people in Myanmar have a limited understanding of sexual and reproductive health, with 38 per cent of adolescents admitting they did not know a woman could become pregnant if she has sex only once, and only 16.67 per cent of young people aged 15 - 24 having accurate HIV prevention knowledge.
To address these issues, UNESCO Yangon, in collaboration with the Ministry of Education, held a policy seminar on 22 March, 2019. More than 50 representatives from Government and non-Government organizations came together to share good practices and identity opportunities for strengthening sexuality education policy, curriculum and teaching in Myanmar.
The event featured the launch of the Myanmar-language version of the 2018 revised International Technical Guidance on Sexuality Education (ITGSE), developed by UNESCO, in partnership with the World Health Organization, UNICEF, UNFPA, UNAIDS, and UN Women. The Technical Guidance assists education, health and other relevant authorities in the development and implementation of sexuality education programmes and materials.
UNESCO regional advisor for health and education, Kabir Singh, said the UN Technical Guidance covers a wide range of topics; going beyond sexual and reproductive health to include broader life skills such as negotiating consent and staying safe.
“While young people in Myanmar face challenges in accessing sexual and reproductive health (SRH) information and services, the situation is further exacerbated by social and gender norms that prevent children and young people, particularly girls and other vulnerable groups, from achieving good health and well-being,” he said.
“This is why it is critical that CSE programmes begin at the ages of 5 – 8, as outlined in the UN Technical Guidance. We need to help children at the earliest ages understand gender equality, healthy relationships, and respect for themselves and one another.”
Sexuality education in Myanmar
The National Life Skills Education curriculum in Myanmar, developed by the Ministry of Education (MoE) in collaboration with UNICEF, has been part of the core curriculum in primary schools since 2006, and in middle schools as a compulsory co-curricular subject since 2008. The lower secondary curriculum (grades 5-8) covers seven themes, including reproductive health, HIV and STIs, substance use, and disease prevention and nutrition.
A 2012 assessment of Life Skills Education in middle school found that knowledge around reproductive health was low, with the authors suggesting that cultural sensitivity and lack of teacher training may be contributing factors. A recent UNICEF U-Report, a free SMS social monitoring tool for youth participation in Myanmar, also found that most survey respondents learned about sexuality education through social media, a source that is often not scientifically accurate or age-appropriate.
At the 2019 UNESCO-led policy seminar, Myanmar government representatives agreed to review Life Skills Education in the context of the UN Technical Guidance, ensuring the sexuality education being delivered is comprehensive and age-appropriate. Representatives also indicated that comprehensive sexuality education should be strengthened as part of current education reforms to the basic education curriculum and pre-service teacher education curriculum.
Min Jeong Kim, Head of UNESCO Myanmar Project Office, welcomed the close working relationship between UNESCO and the Ministry of Education in introducing comprehensive sexuality education into the education system.
“The Ministry of Education has shown strong leadership in their efforts to address the challenges faced by children and young people, such as gender inequalities, and sexual and reproductive health. UNESCO shares this commitment to positively impact young people’s lives and look forward to continuing to work in partnership the curriculum core team and the Teacher Education Colleges to integrate CSE into the new curriculum for teacher education,” Min Jeong Kim said.
Delegates at the policy seminar discussed ways in which to introduce comprehensive sexuality knowledge and related life skills to current and future generations of children and young people in Myanmar. The seminar provided a platform that bridged key stakeholders such as public service providers, development partners and non-Government organizations, with a view to starting a dialogue on comprehensive sexuality education, understanding the gaps and identifying the best way forward for full implementation.
The revised technical guidance on sexuality education
The original international technical Guidance published in 2009 positioned sexuality education primarily as part of the HIV response. However, while HIV prevention remains important, evidence and practice demonstrate that sexuality education has a much broader relevance to other issues, not only for young people’s sexual and reproductive health but also for their overall wellbeing and personal development.
The revised Guidance presents sexuality with a positive approach, recognizing that CSE goes beyond educating about reproduction, risks and disease. It reaffirms the position of sexuality education within a framework of human rights and gender equality. It reflects the contribution of sexuality education to the realization of several internationally agreed commitments in relation to sexual and reproductive health, as well as the achievement of the goals in the 2030 Agenda in relation to health and well-being, quality and inclusive education, gender equality and women and girls empowerment.
Based on a review of the sexuality education around the world and drawing on best practices in the various regions, the Guidance demonstrates that sexuality education:
- helps young people become more responsible in their attitude and behaviour regarding sexual and reproductive health
- is essential to combat the school dropout of girls due to early or forced marriage, teenage pregnancy and sexual and reproductive health issues
- is necessary because in some parts of the world, two out of three girls reported having no idea of what was happening to them when they began menstruating and pregnancy and childbirth complications are the second cause of death among 15 to 19-year olds
- does not increase sexual activity, sexual risk-taking behaviour, or STI/HIV infection rates. It also presents evidence showing that abstinence-only programmes fail to prevent early sexual initiation, or reduce the frequency of sex and number of partners among the young.
Related
Status of HIV Programmes in Indonesia
24 February 2025
Press Release
Model Drug Law for West Africa presented to ministers of health on the sidelines of the 72nd session of the World Health Assembly
22 May 2019 22 May 2019GENEVA, 22 May 2019—The West Africa Commission on Drugs, UNAIDS and the Global Commission on Drug Policy today presented the Model Drug Law for West Africa to ministers of health of the Economic Community of West African States.
Drug laws in western Africa are not having the intended effect. Neither drug use nor drug trafficking have been effectively reduced. Drug trafficking in western Africa has reached such an extent that the drug trade threatens stability in the region. Data from the United Nations Office on Drugs and Crime from 2014 show that the use of cannabis in western Africa is much higher than globally―12.4% of people in the region had used cannabis in 2014, whereas only 3.9% of the global population had done so―and the problematic use of prescription and synthetic drugs is increasing. The rise in prison populations owing to pre-trial detention and drug-related offences has led to serious prison overcrowding in most countries.
“People who use drugs need help and care, not punishment. Stigmatizing them and locking them up in ever-increasing numbers only worsens health issues and puts enormous pressure on the already over-stretched criminal justice systems,” said Olusegun Obasanjo, former President of Nigeria and Chair of the West Africa Commission on Drugs. “It took our region years to adopt evidence-based policies regarding the response to HIV, and we are now enjoying life-saving successes every year. Our view is that drug policy needs the same pragmatic, health-based and people-centred approach as the HIV response.”
The model drug law provides concrete templates that countries can adapt to reform their drug laws—legal provisions and how they relate to international legal obligations—as well as useful commentary that explains different options and reasons for choosing the proposed legal solution. The model drug law offers a measured way for decriminalizing drug use and possession for personal use by introducing thresholds, thereby allowing people who use drugs to access health services and seek support. The model drug law acknowledges that barriers must also be removed so that the millions of people in need of health services, including people living with cancer or with HIV, can access the treatment and care they need.
“Countries need to take a human rights approach to HIV and drug use and to make sure that the health and well-being of people come first,” said Gunilla Carlsson, UNAIDS Executive Director, a.i., while presenting the report to the ministers of health on the margins of the seventy-second session of the World Health Assembly, being held in Geneva, Switzerland. “We know that harm reduction works, we know that decriminalization works―countries cannot continue to disregard the evidence and urgently need to take action.”
The widespread stigma and discrimination, violence and poor health faced by people who inject drugs are compounded by high rates of HIV. While the incidence of HIV infection globally declined by 25% between 2010 and 2017, new HIV infections among people who inject drugs continue to rise. Of the 10.6 million people who injected drugs worldwide in 2016, more than half were living with hepatitis C, and one in eight were living with HIV.
International experience has shown that it is possible to muster the political will to make these wide-ranging changes to drug laws in order to address the spread of infectious diseases and their burden on development. Ruth Dreifuss, former President of Switzerland and Chair of the Global Commission on Drug Policy, said, “This is a defining moment where governments can turn the tide and control health epidemics by providing the right sets of prevention, treatment and harm reduction tools, or fail to do so if they maintain the prohibitionist status quo.”
Global Commission on Drug Policy
The purpose of The Global Commission on Drug Policy is to bring to the international level an informed, science-based discussion about humane and effective ways to reduce the harm caused by drugs and drug control policies to people and societies.
West Africa Commission on Drugs
Convened by Kofi Annan, the West Africa Commission (WACD) on Drugs comprises a group of distinguished West Africans from the worlds of politics, civil society, health, security and the judiciary. The Commission, chaired by former President Olusegun Obasanjo of Nigeria, is an independent body and can therefore speak with impartiality and directness.
UNAIDS
The Joint United Nations Programme on HIV/AIDS (UNAIDS) leads and inspires the world to achieve its shared vision of zero new HIV infections, zero discrimination and zero AIDS-related deaths. UNAIDS unites the efforts of 11 UN organizations—UNHCR, UNICEF, WFP, UNDP, UNFPA, UNODC, UN Women, ILO, UNESCO, WHO and the World Bank—and works closely with global and national partners towards ending the AIDS epidemic by 2030 as part of the Sustainable Development Goals. Learn more at unaids.org and connect with us on Facebook, Twitter, Instagram and YouTube.
Contact
Global Commission on Drug PolicyEric Grant
tel. +41 79 124 1523
eric.grant@globalcommissionondrugs.org
UNAIDS
Sophie Barton-Knott
tel. +41 22 791 42 37
bartonknotts@unaids.org
Model Drug Law for West Africa
Press centre
Download the printable version (PDF)