





Feature Story
UNAIDS and Luxembourg―working together in western and central Africa
09 October 2019
09 October 2019 09 October 2019Western and central Africa continues to lag behind the rest of Africa in preventing and treating HIV, leaving millions of people vulnerable to HIV infection and 2.4 million people living with HIV without treatment. Following calls to action made at the 2016 United Nations High-Level Meeting on Ending AIDS and the July 2016 African Union summit, UNAIDS and partners launched a plan to accelerate efforts to stop new HIV infections and ensure that everyone in the region has access to life-saving treatment.
Although resources available in western and central Africa to respond to HIV increased by 65% between 2006 and 2016, reaching an estimated US$ 2.1 billion, most countries remain highly dependent on donors. However, international funding is declining and current investment levels are far lower than what is actually needed to make a sustainable change.
Luxembourg is one country that remains committed to investing in western and central Africa. Marc Angel, Chair of the Foreign Affairs and Development Committee in the Luxembourg Parliament and UNAIDS Champion for the 90–90–90 Targets, joined UNAIDS on a recent visit to Senegal to see how Luxembourg’s contribution to UNAIDS for the acceleration of the AIDS response in western and central Africa was helping to make a difference.
Supported by funding from Luxembourg, UNAIDS and partners have established the innovative Civil Society Institute for HIV and Health in West and Central Africa. The institute acts as a coordinating mechanism for around 80 nongovernmental organizations working in the interests of people affected by HIV in 20 countries across western and central Africa.
One such group is CEPIAD, the first centre for harm reduction for people who inject drugs in western Africa. The medical staff and social assistants are pioneers in the region, treating people who use drugs with a public health approach rather than judgement. In Mbour, at the treatment centre for key populations, Mr Angel heard from people who had injected drugs in the past, who shared their personal stories of how the centre had helped them to reintegrate with their families and society.
“Only by including key populations can the 90–90–90 targets be reached,” said Mr Angel. “Senegal’s public and civil society actors have to continue working hand in hand towards this objective. For Luxembourg’s development cooperation, the human rights dimension in the fight against AIDS and in global health is key. Together with UNAIDS we need to ensure that voices from communities are being heard, working all over the country, in particular with vulnerable populations, including children.”
Mr Angel also visited the paediatric treatment ward of the Albert Royer Hospital, where he met young people living with HIV. They shared their experiences of treatment for HIV, which is allowing them to live normal lives. He noted the progress made in stopping new HIV infections among children in Senegal and the important work done around sexual and reproductive health and HIV to prevent new HIV infections among adolescents.
During meetings with the Minister of Health and Social Action of Senegal, Abdoulaye Diouf Sarr, and the Secretary-General of Senegal’s National AIDS Committee, Safiatou Thiam, Mr Angel praised Senegal for decreasing the national HIV prevalence.
However, he also highlighted areas of concern, including the high HIV prevalence among key populations, emphasizing that access to treatment for key populations was instrumental to ending AIDS by 2030. He also advocated for an increase in national resources to respond effectively and sustainably to HIV in Senegal.
Region/country
Related




Feature Story
How London’s first dedicated HIV ward changed the AIDS response
03 October 2019
03 October 2019 03 October 2019Opened in 1987 by Princess Diana, the Broderip Ward at the Middlesex Hospital in London was the United Kingdom’s first ward dedicated to caring for HIV patients. UNAIDS Senior Adviser on Science, Peter Godfrey-Faussett, worked on the Broderip Ward as a newly qualified doctor and remembers it as an intense and highly emotional period.
What are your first memories of HIV?
I was finishing my medical training in London when the first reports of what would subsequently be called HIV and AIDS came out. We had no idea then of the unprecedented nature of what was happening. As a medical student approaching my final exams, my concern was to know the facts, but it was clear to me even then that many of these “facts” were not yet understood. After qualifying, I soon found myself working at the Hospital for Tropical Diseases in London and on the Broderip Ward at the Middlesex Hospital.
How did London’s medical professionals react to this new health challenge?
The organization of services for HIV varied in different parts of London. The staff at the sexual health clinics, or departments of genitourinary medicine, as they were called then, were establishing outpatient services with counselling, support and care for people living with HIV. But these teams were generally not well equipped to provide care for people who had to be admitted to hospital. In each hospital, a different specialist team took on the care of the ever-expanding population of people living with, and dying from, HIV. Many of those needing care had pneumonia, often caused by pneumocystis. Others had persistent severe diarrhoea, neurological problems or skin diseases, including Kaposi's sarcoma.
We had an amazing team led by Steve Semple and worked in close collaboration with the staff at James Pringle House, one of the dedicated sexual health clinics in London. Steve Semple was a respiratory physician with an expertise in the normal regulation of breathing. In other parts of London, the leaders were gastroenterologists, immunologists or infectious disease physicians.
We were all learning quickly how best to care for a wider range of infections, cancers and other conditions, all while coming to understand the social networks and behaviours of our mostly gay patients.
It must have been a difficult time
It was, of course, a hugely sad time. We could treat many opportunistic infections and provide counselling and support, but HIV was almost invariably lethal in those days and we saw so many young men, who were often at the forefront of the lively and creative communities that made London such a great city, fade away gradually or deteriorate more suddenly and die.
As a medical student and young doctor, most of the people that I had treated were reaching the end of full productive lives, but here on the Broderip Ward were people of my own age, reading the same books, going to the same operas and plays. It was often hard to remain clinically detached. I can remember so many of them so clearly. And so many of their loved ones and families.
How did the opening of the Broderip Ward change the way people were cared for?
The nurse in charge of the ward, Jacqui Elliott, was a wonderful woman. Along with Steve Semple, she encouraged us all to break the mould and provide care in a very different way. Back then, hospitals were quite old fashioned and regimented. The matron and the consultant were at the point of a huge pyramid, and often the patients were near the bottom!
Right from the start we engaged with the patients and their partners, and, where necessary, turned a blind eye to regulations. The ward was the only one in the hospital to have additional fridges full of delicious meals that people brought in for their partners, often shared with other patients and the health team!
In those days, there were payphone kiosks at the end of long cold corridors in the hospital and hospital gowns were hideous affairs that tied up loosely at the back. We were the first ward to install a phone on the nurses’ desk so that patients could make calls more easily. We encouraged people to wear their own clothes and dressing gowns and to come and go from the ward as they wished. Everyone on Broderip worked around the clock. Our parties were the ones that everyone in the hospital wanted to come to.
We were learning, and no doubt we made mistakes, but we were certainly among the first medical professionals to listen to our patients and to try to provide what they needed.
And did clinical care change?
The dedicated ward was quickly a focus for teams from all over the teaching hospital. Whenever something new or strange occurred, we had a network of the best specialists in every medical discipline. The weekly clinical meeting attracted clinicians from all over the hospital and from the other hospitals in London and elsewhere.
As a junior doctor it was terrifying having to present each complicated patient to the assembled experts and seek their inputs. But I think the medical care that our patients received was at the cutting edge. We had strong relationships with the psychosocial counselling teams and with the palliative care team, who worked hard to make dying as comfortable as possible. We were, of course, trying out new antiretroviral medicines. Many of our patients were in the early trials of zidovudine, and some patients did improve.
How did patients, their friends and families and staff on the ward cope?
Each patient was an individual with his (or occasionally her) particular relationships with friends, lovers and family. For some, however, admission to the Broderip Ward was the first time that people had acknowledged their sexuality within their family, and they were also having to deal with coming to terms with HIV and the implications of impending death. The staff on the ward had to be constantly aware of who knew what and who could meet whom. Some patients preferred their family not to know on which ward they were being cared for. One of our jobs on the ward was to facilitate disclosure and counsel patients and their partners and families as they came to terms with their situation. We also had a team of make-up artists to help camouflage the visible signs of Kaposi’s sarcoma and dieticians who aimed to optimize people’s nutrition. There was always a strong sense of camaraderie and plenty of opportunities for laughter as well as tears.
How did the United Kingdom’s approach to HIV change in the 1990s and beyond?
The arrival of increasingly effective antiretroviral therapies changed everything. Early treatments were toxic and hard to manage, with specific needs for some pills with food, some without, some needing to be kept in the fridge and some needing an alarm clock to take in the middle of the night. But they worked.
Patients in hospital began to realize that they were not going to die in the next year or two. The United Kingdom’s amazing health system, the National Health Service (NHS), and the wide network of sexual health clinics, meant that professional, high-quality care and treatment was accessible to everyone at no cost. London has always been a centre for travel and migration and the diagnosis and treatment of sexually transmitted infections were exempt from any questions about residence or immigration status. Even for hospital care, the rules could be interpreted to allow everyone to be treated.
The other huge development was that grass-root community organizations sprung up and were funded. People among the African diaspora supported each other and became more organized and vocal. Services in different parts of London catered to different population bases, so that in our hospital many of our patients were gay men, whereas in east London there was a much larger population of women, usually African. Inevitably, people's challenges reflected the social context in which they lived, as well as the gender-specific clinical aspects of HIV.
More recently, some of the systems that made the United Kingdom so open to people living with HIV have changed. Funding for the sexual health clinics and community organizations is tighter, and the restrictions on who is eligible for NHS treatment are enforced more rigorously. On the other hand, most United Kingdom cities remain vibrant, tolerant places and the gay community especially has pushed for earlier and better diagnosis, treatment and prevention. Stigma is certainly still there, but I believe most people can find a clinic and a team that welcomes and supports them through the challenges of living with HIV.
There is such an array of treatment and prevention options available today, is the HIV epidemic over in the United Kingdom?
We are making exciting progress, and each year sees a fall in the number of new HIV infections, particularly in London and the other big cities. Outbreaks will continue, recently among people who inject drugs in Scotland. Ongoing stigma and denial prevent people from all communities, and particularity the African diaspora, from getting tested and accessing effective treatment or prevention promptly.
And, of course, people need treatment for life. So even as the number of new infections falls, we will need ongoing care and support and good surveillance for many more years.
Region/country
Related






Feature Story
The pros and cons of being small
27 September 2019
27 September 2019 27 September 2019Being small has its advantages. In most Caribbean countries, a local clinic or hospital isn’t very far away. Strong primary health-care systems and high levels of health-care access for pregnant women are at the heart of the region’s success in preventing new HIV infections among children. Seven Caribbean islands have been validated by the World Health Organization as having eliminated mother-to-child transmission of HIV. They range from the British overseas territory of Montserrat, with a population of 5000, to Cuba, home to more than 11 million people.
Antigua and Barbuda received its elimination of mother-to-child transmission of HIV validation in 2017. According to its Chief Medical Officer, Rhonda Sealey-Thomas, the Ministry of Health devised strategies to make certain that all pregnant women feel empowered and supported to start antenatal care as early as possible. The twin-island state employs a community nursing model in which district nurses conduct home visits to encourage women to go to health centres near the start of their pregnancies and to keep their appointments. The country uses its 26 community clinics to ensure that every woman had easy geographical access to antenatal care.
In the Bahamas, the Ministry of Health and the wider AIDS response are working towards validation. It was among five Caribbean countries that achieved 100% coverage for early infant diagnosis in 2018.
Nikkiah Forbes, Director of the National HIV/AIDS and Infectious Disease Programme at the Bahamas Ministry of Health, points to the importance of having a robust health-care system with available and free antenatal care and strong laboratories. Antenatal care is universal in the Bahamas and available at community clinics throughout the island chain. Mothers are encouraged to access care as early as possible and an HIV test is offered during the first visit. Laboratory screening is repeated at 32 weeks. Dedicated nurses ensure that all mothers and infants are retained in care and receive the additional support they need.
“You have to get out in the field if you are going to provide HIV care. We go to clinics to meet the women so we can provide support and counselling. We go into the field and test their partners. We really follow up to ensure they come to the clinic, feel comfortable and are expedited. We ensure they are getting their medication, all their labs are in and that they have nutrition support. If they don’t come to us,” one nurse explained, “we go to them.”
But a small population size also comes with challenges. For migrants, there is often the added vulnerability of standing out when accessing services. Antigua and Barbuda provides health care to all migrants. “Services in the community health clinics are free of cost. Nationality does not matter. If migrants are not afforded health care, it costs more in the long run. By protecting the health of migrants, you are indirectly protecting the health of your own population,” Ms Sealey-Thomas explained.
In the Bahamas, there are also mechanisms for Haitian migrants to access care. “We have translators that speak Haitian Creole at a one-stop-shop clinic. Translations of education materials are also available in Haitian Creole,” said Ms Forbes.
But for citizens who are members of close-knit communities, special care had to be taken to strengthen confidentiality and address stigma and discrimination in health-care settings. Throughout the region, health-care providers have received anti-stigma and discrimination training to address issues that include unconscious bias and confidentiality.
Still, in any Caribbean country the likelihood of people knowing or recognizing others where they access care is relatively high. It’s a challenge that countries must overcome in order to accelerate results across the continuum of care, for adolescents, women and men alike.



Feature Story
HIV in small island developing states
27 September 2019
27 September 2019 27 September 2019“I am not ready to share my status or disclose myself to the public. I am afraid of being isolated, stigmatized and discriminated against. For me, it’s good for only me to know my status, rather than disclose it to other people,” said Mara John (not her real name), who comes from a Pacific island and is living with HIV. Similar stories of isolation, self-stigma, poverty and lack of human rights can be heard from many people living with HIV in small island developing states (SIDS).
On 27 September, United Nations Member States meet for a high-level review on SIDS at the United Nations General Assembly in New York, United States of America. In his report published ahead of the summit, the United Nations Secretary-General highlights that SIDS, particularly Caribbean SIDS, continue to be challenged with “high levels of youth unemployment, poverty, teenage pregnancy, and high risk for HIV infection.”
A group of 38 countries, including islands in the Pacific, the Caribbean and elsewhere, the SIDS have been provided with dedicated support owing to the specific constraints they face―for example, the size of their territory, remoteness or exposure to climate change―as a result of the United Nations Conference on Sustainable Development, also known as Rio+20, held in June 2012. In 2014, the SIDS Accelerated Modalities of Action Pathway was adopted by United Nations Member States to outline actions for sustainable development in the SIDS, including a commitment to achieving universal access to HIV prevention, treatment, care and support and to eliminating mother-to-child transmission of HIV.
While the SIDS have seen progress, there are wide differences between, for example, Cuba, the first country globally to be certified as having eliminated mother-to-child transmission of HIV, in 2015, and Mauritius, where 30% of people who inject drugs are reported to be living with HIV.
“The Sustainable Development Goals highlight the importance of leaving no one behind. This is particularly meaningful for people living with HIV in small island developing states, who face isolation, stigma and discrimination and inequalities. We need to do more to ensure that they receive the services they need,” said Gunilla Carlsson, UNAIDS Executive Director, a.i.
Generally in small islands, key populations, including gay men and other men who have sex with men, transgender people, sex workers and people who inject drugs, bear a disproportionately high burden of HIV. In some SIDS, however, HIV also significantly impacts the general population―while key populations and their sexual partners accounted for 47% of new HIV infections in the Caribbean in 2018, more than half of all new HIV infections were among the general population. Stigma and discrimination by health-care workers is still a major challenge in the Pacific. For example, 60% of female sex workers surveyed in Fiji reported avoiding HIV testing owing to fear of stigma from health-care providers, as did more than 30% of gay men and other men who have sex with men.
Another aspect that SIDS have in common is the strength of communities of people living with HIV and the presence of exceptional political will, often at the highest levels. Ratu Epeli Nailatikau, the former President of Fiji and current Speaker of the Fiji Parliament, has been speaking out against stigma and discrimination for many years.
Networks of people living with HIV and of key populations are at the centre of the movement to end AIDS in the SIDS. In the Pacific, people living with HIV came together to publish a report in 2018 describing their situation in their own words. Similarly the Mauritius Network of People Living with HIV has provided vocal leadership to the response and clearly outlines the challenges of the community in its 2018 People Living With HIV Stigma Index report. In the Caribbean, the late activist and academic Robert Carr is credited for helping to shape global thought around the importance of addressing the human rights of vulnerable and marginalized communities as part of the AIDS response. In 2005, he helped to establish the Caribbean Vulnerable Communities Coalition, which works on behalf of the groups most often left behind.
UNAIDS is working to support SIDS through its team for the Caribbean, based in Jamaica, for the Pacific islands from its Fiji office and for the Indian Ocean islands from the UNAIDS office in the Seychelles. Priority is given to SIDS with a higher prevalence of HIV, through programmes targeting the most vulnerable populations.
Small Island Developing States

Feature Story
Without sustainable financing the AIDS response will fail
26 September 2019
26 September 2019 26 September 2019This week, the United Nations General Assembly committed itself to achieving universal health coverage by 2030. It also pledged to accelerate efforts to achieve the Sustainable Development Goals, including ending AIDS, by 2030. Those commitments show that there is political will to respond to the gravest crises facing the world.
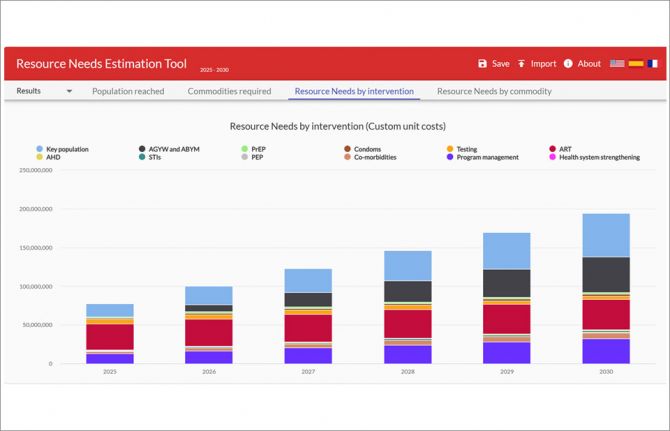
In 2016, the General Assembly agreed, in the Political Declaration on Ending AIDS, to a steady scale-up of investment in the AIDS responses in low- and middle-income countries, increasing to at least US$ 26 billion by 2020. At the end of 2018, however, only US$ 19 billion (in constant 2016 US dollars) was available. And, worse, that US$ 19 billion was almost US$ 1 billion less than a year before.
Instead of a steady increase, global financing for HIV is decreasing. The political commitment is simply not being matched with the financing required to turn the vision of an end to AIDS into reality. With a little more than a year to go until the 2020 target of US$ 26 billion, finance for the AIDS response falls short by US$ 7 billion. This shortfall is particularly alarming because we know that investments in the AIDS response save lives―investing in the AIDS response is a great investment.
“The world can’t afford to backslide on investment in the AIDS response,” said Gunilla Carlsson, UNAIDS Executive Director, a.i. “Countries must honour their pledge to steadily increase their investment in the response to HIV if the world is to meet its obligations to the most vulnerable and disadvantaged.”
Funding declines were seen in all sectors in 2018: domestic resources (a 2% decline), the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund) (a 20% decline, explained by fluctuations in its three-year grant cycle), other multilateral channels (a 2% decline), the Government of the United States of America’s bilateral programmes (a 3% decline), the bilateral programmes of other donor countries (a 17% decline), philanthropic organizations (an 18% decline) and other international sources (a 4% decline).
Low- and middle-income countries are increasingly financing their AIDS responses themselves. Between 2010 and 2018, domestic resources invested by low- and middle-income countries in their AIDS responses increased by 50%, while international investments increased by just 4%.
Domestic financing in 2018 in low- and middle-income countries accounted for 56% of total financial resources, although there were wide variations among regions. In eastern and southern Africa, the region with the highest HIV burden, 59% of HIV resources came from donors in 2018―this rises to 80% if South Africa is taken out of the analysis. Between 2010 and 2018, all major donors except the United States reduced their bilateral direct contributions to the AIDS responses of other countries.
This October is a critically important time for finance and HIV. In Lyon, France, on 10 October, governments and other partners will meet for the Global Fund’s sixth replenishment pledging conference. Seeking to raise at least US$ 14 billion for the response against HIV, tuberculosis and malaria for 2020–2022, the Global Fund estimates that 16 million lives will be saved by its programmes if fully funded, building on the 27 million lives saved since its inception in 2002.
“I urge countries to fully fund the Global Fund to Fight AIDS, Tuberculosis and Malaria in its upcoming replenishment―16 million men, women and children are counting on it,” said Ms Carlsson.
Related information




Feature Story
Communities of faith―helping to find the missing men and seeking justice for children
26 September 2019
26 September 2019 26 September 2019Bobby was born in 1996 in the small, mountainous country of Lesotho. His mother was living with HIV, and, unknown to him, he was born with the virus. He lost his little brother when he was just four years old and his little sister when she was just six to meningitis—a devasting blow to Bobby. Life was hard, and at 12 years old he received news that was to change his life forever. He was diagnosed with tuberculosis and found out that both his mother and father were living with HIV.
But Bobby didn’t give up. “Some people wanted to break me, but they only made me stronger. Some people wanted to exploit me, but they only made me smarter,” said Bobby. “Taking pills and going from an HIV-positive child to an HIV-positive activist has not been easy. I faced a lot of stigma and discrimination. But one of my biggest dreams is to live and to contribute, which is why I’m here today.”
On 26 September, Bobby shared his journey with an audience of more than 150 faith leaders and partners working on HIV at the Communities of Faith Breakfast, held at the Yale Club, on the sidelines of the United Nations General Assembly in New York, United States of America.
Bobby’s story and the thousands of others like his have inspired faith groups around the world to take action to stop new HIV infections and support people living with and affected by the virus. Speaking at the event, the Minister of Health of Zambia, Chitalu Chilufya, shared how faith leaders in his country are playing an important role in improving the health and well-being of their congregations, particularly by reaching men.
“We have several ministers that hold health Sundays, bringing in doctors to engage their congregation on health matters,” said Mr Chilufya. “Men are in the marketplaces and men are in the churches—and this is how we are reaching them. Through these efforts we have seen the percentage of men who have not been tested for HIV reduce from 50% to 30%.”
The importance of reaching men was echoed by many of the speakers, as was the urgent need to ensure that children have access to optimal HIV services and justice.
“In 2018, we lost 100 000 children to AIDS-related deaths and only 54% of the 1.7 million children living with HIV worldwide were accessing treatment. These are very sad statistics,” said Gunilla Carlsson, UNAIDS Executive Director, a.i. “Engagement of faith-based health partners will be critical to help governments transform their commitments on HIV into real action on the ground.”
The breakfast provided a space for partners to come together and share ideas and experiences of innovative approaches to reach young men, adolescent girls and young women and children living with HIV with HIV prevention and treatment services. It also fostered positive discussions on how to prevent and respond to sexual violence against children, which significantly increases their risk of HIV infection.
“Our discussions here will shed light on what is possible and once we know what is possible there is no excuse to make it possible for everyone, everywhere, at all times,” said Deborah Birx, United States Global AIDS Coordinator and Special Representative for Global Health Diplomacy.
Related




Feature Story
Young people taking action, inspiring change
25 September 2019
25 September 2019 25 September 2019Around 19 000 inspirational young people gathered at WE Day UN on 25 September to celebrate the incredible work they are doing to make positive change in their communities and around the world. All the young people who attended the event had earned a free ticket by taking action on one local and one global cause of their choice. Taking place in New York, United States of America, during the seventy-fourth session of the United Nations General Assembly, this year’s WE Day UN was held in partnership with UNAIDS, the UN Global Compact and UN Women.
UNAIDS has enjoyed a long-standing partnership with WE Day, helping to educate young people about HIV and to support them in their socially conscious efforts to make a sustainable impact in their societies and around the world. Through the important work of WE Day, UNAIDS is able to reach more than 20 000 schools across the United States, the United Kingdom and Canada.
Speaking to the young audience in the Barclays Center Stadium in New York, Gunilla Carlsson, UNAIDS Executive Director, a.i., said, “AIDS is not over, but it can be! You can be the generation that ends AIDS and leads the world in achieving the Sustainable Development Goals, creating a better world for generations to come.”
Ms Carlsson used the opportunity to remind young people of the importance of achieving the Sustainable Development Goals and how critical it is to talk about HIV to break down the stigma around the epidemic. Her remarks were preceded by a newly released animation from UNAIDS that demonstrates the interlinkages and interdependence of HIV and the Sustainable Development Goals and how efforts to end AIDS can lead to a wider, people-centred social transformation.
Related





Feature Story
Making a difference in Ethiopia one district at a time
24 September 2019
24 September 2019 24 September 2019Ethiopians travelling to seek medical care outside the country cost the Ethiopian economy US$ 250 million per year. Around 40% of Ethiopia’s health centres have no electricity and 50% are without access to clean water. But despite these challenges, Ethiopia is striving to improve its health-care system so that it can meet the needs of all its citizens, in line with the global commitment made at the United Nations General Assembly High-Level Meeting on Universal Health Coverage on 23 September to achieve universal health coverage by 2030.
Ethiopia has taken an innovative approach to managing priorities and is setting ambitious targets. Finding new technologies and innovations for the health, energy and other sectors is critical.
The government will launch a programme in October that will see 10 ministries work together to define and address priorities on a district-by-district level. This will require partnership across the private sector, communities and international development partners. The Ethiopian Minister of Health, Amir Aman, is committed to making a change by working with UNAIDS and other international partners to identify and apply the right innovations.
“I appreciate the commitment of UNAIDS and the Health Innovation Exchange to support Ethiopia in the use of innovation, especially for tuberculosis, HIV, hepatitis B diagnosis, the use of solar panels for health facilities and incorporating artificial intelligence to fast-track access to health-care services, as well as facilitating local production of medicine and medical supplies,” said Mr Aman.
This partnership with UNAIDS was sparked when Mr Aman visited the innovation exhibition at the launch of the UNAIDS-led Health Innovation Exchange platform in Geneva, Switzerland, in May. The Health Innovation Exchange is a platform led and founded by UNAIDS that identifies the challenges faced by health providers and connects them with high-impact innovations. It also links with investors to scale up innovations and develop sustainable solutions.
Mr Aman challenged the Health Innovation Exchange to work with the country to identify a variety of potential solutions to its priorities and to facilitate connections across the government and local partners. UNAIDS brought together a delegation of innovators and investors in Ethiopia from 3 to 6 September to explore opportunities for integrating innovative solutions and technologies for health into the country’s development efforts. The delegation included innovators and companies that brought solutions in various areas, such as HIV and tuberculosis diagnostics, solar energy for health-care settings, artificial intelligence for diagnostics and research, pharmaceutical manufacturing and needle safety in hospitals, as well as blended education models to build the Ethiopian health workforce.
The solar energy solutions proposed by members of the Health Innovation Exchange delegation were welcomed, as access to efficient modern energy is a critical enabler for essential maternal and newborn health services. Without energy, many life-saving maternal health services cannot be utilized effectively, which poses critical barriers to reaching the maternal mortality targets and other heath targets of the Sustainable Development Goals.
“Through UNAIDS’ facilitation, we have made direct connections with key ministers and decision-makers in Ethiopia. We have been able to map out a way ahead in bringing technology with potential for impact to Ethiopia and the African market. We are committed to making a difference and appreciate the energy and leadership of the Ethiopian Government in driving such unprecedented change,” said Mauro Pantaleo, Chief Executive Officer, P&P Patents and Technologies.
Meeting with the delegation, Mr Aman committed to supporting the integration of a number of the proposed solutions into the country’s programmes, ensuring that policies and processes will support the new private sector partners working with the country.
Related information

Feature Story
Botswana extends free HIV treatment to non-citizens
24 September 2019
24 September 2019 24 September 2019The Government of Botswana has decided to extend free HIV treatment to foreign residents in a major policy shift that closes a significant gap in the country’s response to the epidemic. The President of Botswana, Mokgweetsi Masisi, announced the intended shift in policy last month after the issue was raised by the Champions for an AIDS-Free Generation in Africa during their visit to the country.
There are an estimated 30 000 foreign residents living with HIV in Botswana, but less than a quarter of them currently have access to treatment. Many foreign residents are simply unable to afford medicines or return home to seek medical help.
Botswana has the third highest HIV prevalence in the world, with more than one in five of the adult population aged 15–49 years living with the virus. In 2016, the country decided to adopt a treat all strategy by extending free treatment to all citizens living with HIV, a step that has been yielding significant results. Since 2010, AIDS-related deaths have decreased by a third, with new HIV infections down by 36% over the same period.
“I commend Botswana for extending free treatment to foreign residents living with HIV,” said Gunilla Carlsson, UNAIDS Executive Director, a.i. “This measure will save lives and help the entire country progress towards ending the AIDS epidemic―it is another example of Botswana’s leadership and its determination to leave no one behind in the response to HIV.”
The Botswana Ministry of Health and Wellness consulted closely with UNAIDS, the United States President’s Emergency Plan for AIDS Relief, the International Organization for Migration, other United Nations agencies and other development partners to develop the new policy.
Based on the government’s decision, the Ministry of Health and Wellness will issue a special government directive to allow health facilities to provide treatment to all people living with HIV residing in the country.
Region/country



Feature Story
Reduce, reuse, recycle: young Ghanaians say yes to less
20 September 2019
20 September 2019 20 September 2019Young people in Ghana have committed to help promote a sustainable environment by reducing the amount of waste they generate, both at home and in school.
“Reduce, reuse, recycle,” was the theme when the advocates met the UNAIDS Ghana Country Director, Angela Trenton-Mbonde, in Accra, Ghana. The advocates took turns to make personal pledges to adopt better waste management practices in order to promote environmental sustainability.
“I commit to acquiring a personal reusable water bottle and to avoiding single-use plastic bottles. This, I believe, will safeguard the planet for everyone,” Pricilla Addo said.
Another advocate, Samuel Nyarko, said, “I pledge to personally ensure that waste generated in my household is well separated so that plastics can easily be collected and recycled. I will educate my schoolmates and community to do the same.”
Ms Trenton-Mbonde encouraged the young people to ensure that their commitments to the planet are fulfilled. “For a sustainable environment, each of us must take personal responsibility and make one commitment, no matter how small and insignificant it may seem in the beginning, because in the end we are all connected: people and planet,” she said.
The youth advocates comprised young people from Hope for Future Generations, a Ghanaian not-for-profit nongovernmental organization focused on empowering women, children and youth.