Feature Story
Closing the HIV prevention investment gap
28 November 2016
28 November 2016 28 November 2016Despite the progress made against HIV over the past 15 years and the availability of proven prevention and treatment methods, the annual number of new HIV infections among adults has remained static, at an estimated 1.9 million a year since 2010. Moreover, there has been resurgence of new HIV infections among key populations in some parts of the world.
Inadequate investments in prevention and unfocused investments that do not reach the most affected populations and locations are among the reasons for the prevention gap. An analysis of four countries in different regions and with different types of epidemic found that the funding of effective and focused primary HIV prevention programmes was low—6% of total HIV investments in Brazil, 4% in Cameroon, 15% in Myanmar and 10% in South Africa. Country allocations for HIV primary prevention (excluding mother-to-child transmission of HIV and voluntary HIV testing and counselling) by the United States President’s Emergency Plan for AIDS Relief and the Global Fund to Fight AIDS, Tuberculosis and Malaria have accounted for roughly 15% of total HIV expenditure.
With funding for prevention falling behind funding for treatment, fewer than one in five people at higher risk of HIV infection today have access to prevention programmes. UNAIDS modelling has shown that investing around a quarter of all the resources required for the AIDS response in HIV prevention services would be sufficient to make possible a range of prevention programmes, including condom programmes, pre-exposure prophylaxis, voluntary medical male circumcision, harm reduction, programmes to empower young women and girls, and mobilizing and providing essential service packages for and with key populations.
Investing more in prevention will also support treatment programmes to achieve their targets. Prevention programmes—including providing HIV information, condom distribution and outreach to young people and key populations—are often the first entry point for individuals to HIV testing and treatment. Community peer-led prevention programmes are also critical for reducing stigma and discrimination. Meanwhile, expanded access to treatment gives people at higher risk choices and encourages them to find out their HIV status; this, in turn, provides the opportunity to retain people who test negative in ongoing prevention programmes. Reducing the number of people who acquire HIV and will need treatment makes antiretroviral therapy programmes more sustainable.
In December 2015, the UNAIDS Executive Director, Michel Sidibé, called for investing a quarter for HIV prevention. In June 2016, United Nations Member States committed in the 2016 Political Declaration on Ending AIDS to ensuring that financial resources for prevention are adequate and constitute no less than a quarter of AIDS spending globally on average.
A number of countries have already taken action to increase their domestic funding for HIV prevention, including Namibia, which has committed to investing 30% of its HIV budget in preventing HIV among adults and children.
Hands up for #HIVprevention — World AIDS Day campaign
Publications


Feature Story
Youth and innovation shine on World AIDS Day in Algeria
01 December 2016
01 December 2016 01 December 2016A dynamic AIDS response characterized by partnership and passion across all sectors, and prioritizing youth and innovation, was celebrated in Algeria on World AIDS Day.
At a lively World AIDS Day commemoration filled with colour and song held in Algiers, key actors in Algeria’s AIDS response came together to reflect on the county’s successes, consider ongoing challenges and emphasize commitment towards ending AIDS by 2030.
Reacting rapidly to the challenges of HIV, Algeria’s response has consistently prioritized cross-sectoral action, community involvement and evidence and innovation within its strategies and policies. Significant results include a sustained low-level epidemic and free provision of antiretroviral therapy for 90% of people living with HIV.
“Algeria has been a pioneer on AIDS in the region, and the response remains highly dynamic. Continued innovation—particularly through harnessing the power of the young, vibrant population—is maximizing gains made and contributing to broader development and rights outcomes,” said UNAIDS Deputy Executive Director Jan Beagle, who welcomed Algeria as a new member of the UNAIDS governing body, the Programme Coordinating Board, from 2017.
To build on the gains made, Ms Beagle noted areas for increased focus, including: access to services for the prevention of mother-to-child transmission of HIV; greater investment in programmes for key populations; and prioritization of women, girls and young people. “Sustained leadership, integration, evidence and rights-based and people-centred approaches that are adaptable at all stages in the life cycle are needed. Let us build on the progress made and continue to be passionate partners in Algeria’s collective efforts,” she said.
Emphasizing commitment to mobilize an accelerated response towards an AIDS-free generation, Ministry of Health Secretary-General Ali Rezgui said, “Young people are this country’s greatest asset. We must treasure them, listen to them and equip them with education, knowledge and tools to prevent HIV and drive forward Algeria’s AIDS movement.”
“Today we celebrate determination, perseverance and progress driven by a highly multisectoral, inclusive response. This model of joint action is critical for the achievement of the interconnected Sustainable Development Goals,” said Eric Overvest, United Nations Resident Coordinator in Algeria.
Commitment to continued collaboration and dynamism was evident through the active participation of young people at the World AIDS Day celebration. “It’s our dream to protect the world against HIV. With solidarity, prevention and knowledge, together we can end AIDS,” a group of schoolchildren sang loudly and clearly.
Region/country

Feature Story
Viet Nam opens its first opioid substitution therapy service for prisoners
25 November 2016
25 November 2016 25 November 2016“In 2010, I participated in a study visit to learn about prison-based methadone programmes in Spain. Witnessing the positive impacts of the programme on prisoners as individuals and prisons as a whole, I reported the results and recommendations of the visit to the Ministry of Public Security,” said Nguyen Xuan Truong, Chief Prison Officer at Phu Son Prison. “It has been quite a wait since then, but I am happy that Phu Son is the first prison in Viet Nam to provide methadone services for prisoners.”
The launch of the pilot opioid substitution therapy service in Phu Son Prison marks a significant milestone in the efforts of the United Nations Office on Drugs and Crime (UNODC) and the Government of Viet Nam for HIV prevention, treatment and care in Viet Nam’s prisons.
“Since 2009, the United Nations Office on Drugs and Crime has worked with the Government of Viet Nam to provide opioid substitution therapy as part of a comprehensive HIV service package for people who are living and working in prisons,” said Christopher Batt, UNODC Officer-in-Charge.
Opioid substitution therapy is an evidence-informed service for opioid dependence. It reduces opioid use by eliminating withdrawal symptoms and drug craving, decreasing the risk of the transmission of HIV or other bloodborne infections and criminal behaviour. In addition, it integrates the patient into a continuum of care during and after his or her stay in prison.
“The opioid substitution therapy service unit is expected to enhance the quality of life of prisoners, reducing transmission of HIV and other diseases and decreasing the rate of relapse and overdose in prison settings,” Mr Batt added.
The Viet Nam Ministry of Public Security estimates that three out of 10 prisoners use drugs.
Prisoners are at higher risk of becoming infected with HIV or other bloodborne infections, including viral hepatitis B or C, relapse or overdose if their treatment needs are not met.
A second opioid substitution therapy service unit will soon be launched in Thanh Xuan Prison, and there are plans for the service to expand to other prisons.
Hands up for #HIVprevention — World AIDS Day campaign
Region/country




Feature Story
Implementing comprehensive HIV and STI programmes with men who have sex with men in Kyrgyzstan
23 November 2016
23 November 2016 23 November 2016In August 2016, the United Nations Population Fund (UNFPA), the Eurasian Coalition on Male Health and Kyrgyz community organizations and civil society partners organized the first ever training on the new guidance on implementing comprehensive HIV and sexually transmitted infection (STI) programmes with gay men and other men who have sex with men in Bishkek, Kyrgyzstan.
The new guidance is the basis of programming for gay men and other men who have sex with men. It was developed through a consultative process led by UNFPA, other United Nations organizations and the Global Forum on MSM and HIV.
Working on HIV and STI prevention, treatment, care and support is deeply challenging in much of eastern Europe and central Asia. Gay men and other men who have sex with men are subjected to considerable harassment, violence, stigma and discrimination. Most men who have sex with men are socially and culturally forced to marry women and face social exclusion and family rejection if they choose to be open about their sexuality. Sex between men is clandestine and opportunities to meet, socialize and love are limited. Empowering all men who have sex with men to live with dignity, free from violence and with affordable and accessible HIV and STI prevention and treatment services is at the heart of the guidance.
The two-day training of trainers in Bishkek brought together members of civil society keen to work on rolling out the guidance—it included a general overview of the document as well as detailed presentations on each of the six chapters. The participants discussed the existing country situation and how programmes focusing on men who have sex with men and contributions to future advocacy actions could be improved.
Thanks to the hard work of the training organizers and the dedication and enthusiasm of the training participants, the Bishkek training was an overwhelming success. The materials and methods used during the training will form the basis for the development of a new training module. The training module, along with the guidance document itself, will be rolled out in countries and its recommendations will be taken into account in the development and implementation of HIV programmes focusing on men who have sex with men across the region.
Hands up for #HIVprevention — World AIDS Day campaign
Region/country
Related
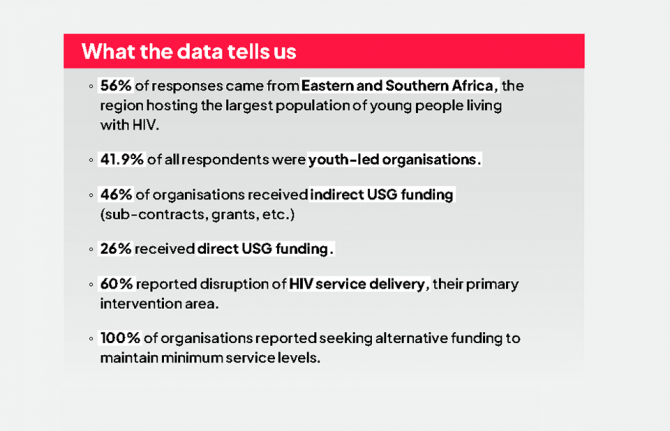
 Multisectoral resilience to funding cuts in Guatemala
Multisectoral resilience to funding cuts in Guatemala
22 December 2025





Feature Story
UNAIDS appoints renowned actor Huang Xiaoming as Goodwill Ambassador for China
28 November 2016
28 November 2016 28 November 2016UNAIDS China has appointed the actor and humanitarian Huang Xiaoming as a UNAIDS National Goodwill Ambassador for China. The announcement was made on 28 November at an event at the UNAIDS office in Beijing, China.
“Huang Xiaoming is an inspiration for millions of people,” said Catherine Sozi, UNAIDS Country Director for China. “I am thrilled that he will leverage his platform as a gifted actor, entrepreneur and philanthropist to help end the AIDS epidemic by 2030. His efforts can re-energize HIV prevention and transform many lives in China and beyond.”
The nomination ceremony included a panel discussion with young people on HIV prevention. The football champion and UNAIDS National Goodwill Ambassador for China, Shao Jiayi, participated in the event and gave congratulatory remarks.
In his new role, Mr Huang will raise awareness on the importance of universal access to HIV prevention, treatment, care and support, with a special emphasis on HIV prevention among young people. Immediately after his appointment, the star showed his support for the UNAIDS global “Hands up for #HIVprevention” campaign, which has been taking place in the lead-up to World AIDS Day on 1 December. Mr Huang posed for photographs with an HIV prevention message written on the palm of his hand. People around the world have been sharing similar photographs and messages through social media.
“I am honoured by this appointment as a UNAIDS Goodwill Ambassador for China,” said Mr Huang. “I am glad that I can play at a least a small part in helping to intensify efforts on HIV prevention. My hope is that young people understand the need to take proper measures to protect not only their own health but the health of the people they love.”
Chinese authorities say there were 654 000 people reported to be living with HIV in China by the end of September 2016. Young people are particularly vulnerable to HIV. Thirteen young people (age 15–24) are infected with HIV every hour in Asia and the Pacific.
Region/country

Feature Story
Protecting the confidentiality and security of personal health information
23 November 2016
23 November 2016 23 November 2016Health services are being scaled up in many low- and middle-income countries. This has resulted in a substantial increase in the amount of personal health information collected in order to develop and maintain comprehensive health records of a person’s use of the services and to monitor and evaluate the use, cost, outcomes and impacts of programmes or services. Detailed personal health information is also needed to evaluate success towards achieving, for example, the 90–90–90 targets, universal health coverage and the Sustainable Development Goals.
However, if personal health information is not held confidentially and securely, people may be reluctant to use health services, owing to fear of being stigmatized or discriminated against. The confidentiality and security of personally identifiable information therefore has to be protected at all levels of the health system. In many countries, this will require the development and implementation of privacy laws and a confidentiality and security framework for protecting personal health information.
Based on the principles of privacy, confidentiality and security, UNAIDS and PEPFAR have developed an assessment tool and an user manual to support countries to assess the degree that the confidentiality and security of personal health information is protected at facility and data warehouse levels and whether national guidelines that include privacy laws exist.
Many countries are in the process of developing and implementing national health identifiers (NHIDs) to ensure that each patient has a unique identity within the health system. This facilitates the development of comprehensive medical records and allows users of services to be tracked across health-care sectors. The development and use of NHIDs in a country’s health-care system promotes the effectiveness and efficiency of data gathering, but their use further underlines the need to protect the confidentiality and security of personal health information.
While policy-makers and other stakeholders in several countries recognize the need to develop and implement policies for protecting the privacy, confidentiality and security of personal health information, to date few countries have developed, let alone implemented, such policies. A workbook has also been developed that can be used to perform the actual assessments in country to assess to what extent policies have been developed and implemented at facility, data warehouse and national levels.
Privacy, Confidentiality and Security Assessment Tool
Related






Feature Story
Sex Workers Academy Africa: increasing demand for rights-based HIV prevention services
21 November 2016
21 November 2016 21 November 2016The Sex Worker Academy Africa is a ground-breaking learning programme that aims to strengthen the rights of sex workers across 47 countries in Africa. It focuses on rapidly scaling up sex worker-led responses to HIV, increasing demand for and access to high-quality rights-based HIV prevention and treatment services for female, male and transgender sex workers and increasing HIV testing, leading ultimately to a fall in new HIV infections among sex workers.
The academy’s curriculum is based on the Sex Worker Implementation Tool. Developed by UNAIDS and partners in 2013, the tool outlines recommendations for the prevention and treatment of HIV and other sexually transmitted infections among sex workers in low- and middle-income countries.
Launched in 2015 and since held several times a year, the academy brings together sex workers from across the continent to explore issues such as community empowerment, addressing violence against sex workers, condom and lubricant programming, community-led services and capacity-building. The curriculum includes knowledge-sharing, art and dance advocacy projects, site visits, thematic workshops and feedback sessions. Each academy lasts a week and includes up to 18 participants.
Since its launch, more than 130 sex workers from 17 African countries have graduated from the academy. It has enabled sex workers from Namibia, the United Republic of Tanzania, Zambia and Zimbabwe to form their own national sex worker networks. In addition, sex workers from Lesotho and Swaziland have organized grass-roots organizations for sex workers where previously none had existed.
The academy is an African Sex Workers Alliance initiative implemented by the Kenya Sex Workers Alliance in Nairobi, Kenya. The curriculum was developed in cooperation with the Ashodaya Academy and the VAMP Institute in India, the Asia Pacific Network of Sex Workers and the Global Network of Sex Workers.
Initial funding for the development of the academy was provided by the United Nations Population Fund and the Dutch-funded nongovernmental organization Bridging the Gaps. Bridging the Gaps and the Robert Carr Fund have provided funding for the ongoing implementation of the academy’s work.
HANDS UP FOR #HIVPREVENTION — WORLD AIDS DAY CAMPAIGN

Feature Story
HIV prevention among key populations
22 November 2016
22 November 2016 22 November 2016Since 2010, the annual global number of new HIV infections among adults (15 years and older) has remained static, at an estimated 1.9 million. Members of key populations, including sex workers, people who inject drugs, transgender people, prisoners and gay men and other men who have sex with men, and their sexual partners accounted for 45% of all new HIV infections in 2015.
In some countries and regions, infection rates among key populations are extremely high—HIV prevalence among sex workers varies between 50% and 70% in several countries in southern Africa. One study from Zimbabwe found HIV prevalence rates of 27% for male inmates, 39% for female inmates and 60% for sex workers, with 9.6% of these getting newly infected between 2009-2014. New infections among gay men and other men who have sex with men have been increasing in all regions in recent years. Across countries, key populations are between 10 and 50 times in greater risk of HIV infection compared to other adults.
Criminalization and stigmatization of same-sex relationships, sex work and drug possession and use, and discrimination, including in the health sector, are preventing key populations from accessing HIV prevention services. Effective government support and community-based and implemented HIV prevention and treatment programmes that provide tailored services for each group are currently too few and too small to result in a significant reduction in new infections.
In order to achieve the target of reducing new HIV infections among key populations by 75% by 2020, a large-scale increase of programmes and the creation of an enabling social and legal environment are needed.
We must reduce new HIV infections among key populations
The global number of new HIV infections among adults has remained static, at an estimated 1.9 million, since 2010, threatening further progress towards the end of the AIDS epidemic.
New HIV infections among gay men and other men who have sex with men are rising globally, and there has been no apparent reductions of new infections among sex workers, transgender people, people who use drugs or prisoners. Studies conducted in southern Africa have found HIV prevalence 10–20 times higher among sex workers than among adults in the general population, with rates of HIV infection reaching 50% of all sex workers tested, and HIV prevalence reaching 86% in one study in Zimbabwe. A synthesis of studies including more than 11 000 transgender people worldwide estimates HIV prevalence to be 19.1%.
Key populations remain among the most vulnerable to HIV. Analysis of the data available to UNAIDS suggests that more than 90% of new HIV infections in central Asia, Europe, North America, the Middle East and North Africa in 2014 were among people from key populations and their sexual partners, who accounted for 45% of new HIV infections worldwide in 2015.
Reinvigorating HIV prevention among key populations requires domestic and international investments to provide key populations with tools, such as condoms and lubricants, pre-exposure prophylaxis and sterile needles and syringes, and testing and treatment. However, the design and delivery of such HIV combination prevention services is often limited by a reluctance to invest in the health of key populations and to reach out to them.
In many countries, key populations are pushed to the fringes of society by stigma and the criminalization of same-sex relationships, drug use and sex work. Marginalization, including discrimination in the health sector, limits access to effective HIV services. There is an urgent need to ensure that key populations are fully included in AIDS responses and that services are made available to them.
Guidelines and tools have been developed for and with the participation of key populations in order to strengthen community empowerment and improve the delivery of combination prevention services by community-led civil society organizations, governments and development partners.
The available evidence shows that when services are made available within an environment free of stigma and discrimination and involving key population communities, new HIV infections have declined significantly. For example, street youth in St Petersburg had a 73% decrease in HIV seroprevalence from 2006 to 2012, primarily due to decreased initiation of injection drug use. This marked reduction in the HIV epidemic among street youth occurred after implementation of extensive support programs and socio-economic improvements.
The replication of such successes and the scale-up of combination prevention programmes in all cities and sites where key populations live and work, implemented by countries and community organization networks, will help prevention efforts get back on track to achieving the target of reducing new HIV infections by 75% by 2020.
Quotes
“WHAT MATTERS IS THE LACK OF INCLUSION AND WIDESPREAD DISCRIMINATION. IT IS CLEAR THAT WE CANNOT END THE AIDS EPIDEMIC WITHOUT TAKING CARE OF THE NEEDS OF KEY POPULATIONS.”
Hands up for #HIVprevention — World AIDS Day campaign






Feature Story
Bringing HIV testing to communities in Cambodia
15 November 2016
15 November 2016 15 November 2016It is nine o’clock in the evening and the night is just beginning in one popular area of Phnom Penh, Cambodia. One multistorey building offers a range of entertainment options: diners enjoy a meal on the ground floor, the bars in the middle level vibrate with popular songs and on the top floor is a hotel.
However, in one corner, next to several karaoke rooms, a serious conversation is taking place. It seems out of context amid the high-pitched laughter, strobe lights, brightly dressed women and male customers. Five entertainment workers are sitting on a sofa talking about why they don’t get tested for HIV.
One woman said, “I don’t know where to go.”
A co-worker agreed and added, “I daren’t go. I am too afraid.”
Their interviewer is 22-year-old Rath Chan Molika. She recently quit her job as an entertainment worker and is now an outreach worker and counsellor with the SMARTgirl programme. She explained why the women working in the karaoke parlour feared public health clinics. “First of all, it’s because they’re scared to go alone,” she says. “Secondly, they’re afraid of the needle and blood.”
There were an estimated 34 000 entertainment workers in Cambodia in 2015, meeting clients in hotels, karaoke parlours, beer gardens, casinos and massage parlours. Unprotected sexual relations with male customers can place some women at higher risk of HIV.
“Some go out with customers without using a condom correctly and consistently. And sometimes they use drugs together, sharing needles and syringes, which increases their risk of HIV,” said Ms Molika.
As part of her job with the SMARTgirl programme, she informs entertainment workers about how to protect themselves from HIV and other sexually transmitted infections and unintended pregnancy. While HIV peer counselling in entertainment establishments has been conducted for a few years, Ms Molika is participating in a highly innovative HIV testing programme.
When the group counselling session ends, she breaks away and in a separate room welcomes Mao Soma. The two women chat quietly for a moment. Ms Molika has been trained to provide pre- and post-HIV-test counselling and to conduct a rapid finger prick test. While Ms Soma winces as the needle pricks her finger, the procedure is over before long. Within 15 minutes there is a result, which suits Ms Soma. “The test is quick and I can get the result immediately,” she says.
Cambodia’s AIDS epidemic is concentrated in key populations
As in many other countries in the region, Cambodia’s AIDS epidemic is concentrated in key populations at higher risk of HIV, which includes entertainment workers, gay men and other men who have sex with men, transgender people and people who inject drugs.
“The government of Cambodia gives importance to collaboration with civil society and also with local people at the community level,” says Ieng Mouly, the Chair of the National AIDS Authority.
Technological innovation in HIV testing
The government, civil society partners and international organizations are now promoting rapid finger prick testing for key populations to replace traditional tests that require laboratory analysis.
“Bringing the facility close to the people is always best. People don’t have to depend on sophisticated laboratory equipment,” explains Ly Penh Sun, the Director of the National Centre for HIV/AIDS, Dermatology and STD.
“The people who are conducting the tests are familiar with the people they are testing. They can interact more. They can support each other,” says Choub Sok Chamreun, of the nongovernmental organization Khana, which provides HIV prevention, care and support services at the community level.
The need for community-based approaches
This community-based HIV testing programme is one of the first of its kind in the Asia and the Pacific region. Across the region, HIV testing coverage among key populations is low. While many countries have scaled up HIV testing in health clinics, representatives of civil society have called for more community-based approaches, focusing on key populations, who often do not attend health clinics.
The results from the Cambodian model are encouraging. Over the past year, implementers reported that more than 36 000 people from key populations were tested, 80% more than in 2014. If a person has a positive reaction on a first rapid screening test, they are accompanied by outreach workers to health facilities for confirmatory tests. Once a medical professional confirms the result, the person has access to HIV treatment.
To improve their efforts to find more people living with HIV, implementation partners are retooling the programme to intensify outreach to people at the highest risk within each key population.
“The plan is to modify the outreach guidelines to the populations at highest risk and intensify targeted outreach activity, as well as active case management, to register and retain the people who were found to be HIV-positive, to ensure they receive treatment,” says Mr Sun.
Hands up for #HIVprevention — World AIDS Day campaign
Region/country

Feature Story
Reducing the impact of HIV among adolescent girls
11 November 2016
11 November 2016 11 November 2016Around 180 young women and adolescent girls from Malawi, Kenya and Uganda have led a pilot project that aims to strengthen the leadership of young women and adolescent girls in the AIDS response. Called Empowerment + Engagement = Equality, the programme aims to build stronger leadership among young women and adolescent girls to engage in national assessments initiated by the All In to #EndAdolescentAIDS platform. The programme addresses issues of gender inequality that heighten adolescent girls’ vulnerability to HIV infection and provides safe spaces where experiences can be shared.
The initiative, designed and implemented by UN Women and the International Planned Parenthood Federation, mobilized more than 1000 young advocates, including young women living with HIV, to voice their concerns at the local, regional and national levels. As well as sharing knowledge among themselves, the participants engaged in face-to-face and online meetings with parents, teachers, religious leaders and other community stakeholders to discuss how to change harmful gender norms and inequalities that increase the risk of HIV infection.
The First Lady of Malawi, Gertrude Mutharik, participated in one of the discussions and committed her support to challenging the issues that increase the risk of HIV infection among young women, including gender-based violence. The young leaders have continued to advocate at the highest levels, taking part in debates at the International AIDS Conference in Durban, South Africa, in July 2016.
“Some of the most fulfilling work I have done as part of this project is to support other girls like me to feel empowered and in control of their lives,” said Divina Kemunto, from Kenya, “I shared my personal experience and encouraged girls living with HIV to believe that they too can walk with their heads held high and a smile on their face.”
Preventing new HIV infections among adolescent girls and young women in sub-Saharan Africa is crucial if the world is to end the AIDS epidemic by 2030—in 2015, 75% of new HIV infections in sub-Saharan Africa among adolescents were among adolescent girls aged 10–19 years. Preventing infections means empowering young women and girls to stay in school so they have better economic prospects, ensuring that they have the knowledge, information and tools to avoid unintended pregnancy and sexually transmitted infections and making sure they know what to do when faced with sexual violence.
Laws and policies that discriminate against women and girls must be dismantled and their sexual and reproductive health and rights must be fully respected.
Hands up for #HIVprevention — World AIDS Day campaign
Related
 “Who will protect our young people?”
“Who will protect our young people?”
02 June 2025