

Feature Story
UNAIDS saddened by the death of Cyriaque Yapo Ako
22 July 2021
22 July 2021 22 July 2021By Brigitte Quenum, UNAIDS Country Director for Côte d’Ivoire
It is with great sadness that I learned on 15 July 2021 of the death of Cyriaque Yapo Ako, one of the pioneers in the response to HIV in Côte d’Ivoire and in Africa as a whole.
A founding member of Ruban Rouge CI in 1994, he never stopped promoting the role of communities in the response to HIV. The Executive Director of RIP+ in the 2000s, he then contributed his expertise to several organizations, including the International Treatment Preparedness Coalition, African Men for Sexual Health and Rights and I CHANGE CI, and collaborated with several partners, including UNAIDS, Population Services International, the United States President’s Emergency Plan for AIDS Relief and the United Nations Development Programme, as a resource person for technical assistance.
As a founding member of Arc-en-Ciel in 2003, the first nongovernmental organization for gay men and other men who have sex with men in the AIDS response in Côte d’Ivoire, he advocated for the need to create a safe space for sexual minorities in Africa, in particular in Côte d’Ivoire, where gay men and other men who have sex with men were commonly subject to stigma, discrimination and violence.
His dynamism and activist spirit enabled him to speak out on behalf of the most marginalized and neglected people in the AIDS response.
From 2004 to 2009, he was the representative of people living with HIV and sexual minorities on the Country Coordinating Mechanism Côte d’Ivoire, where he made a significant contribution to defending people-centred HIV responses in the development of HIV applications to the Global Fund to Fight AIDS, Tuberculosis and Malaria.
His participation in several international conferences contributed to the advocacy of the rights of people living with HIV and more broadly the rights of key populations. He defended his positions, notably through his participation in events such as the International Conference on AIDS and STIs in Africa (ICASA) in 2008 in Dakar, Senegal, ICASA 2011 in Addis Ababa, Ethiopia, ICASA 2013 in Cape Town, South Africa, and the 2016 International AIDS Society Conference in Durban, South Africa, with his contribution in the form of oral presentations and statements.
His passing is a great loss to all those involved in the AIDS response, especially those committed to defending the most vulnerable.
He was a friend, brother and colleague to many of us.
May his soul rest in peace.
Our work
Region/country




Feature Story
Changing the landscape of community engagement in the HIV response in Indonesia
22 July 2021
22 July 2021 22 July 2021“Communities must be allowed to sit in the driver’s seat and take control of their lives. They are not passengers that sit idle, but leaders capable of making changes,” said Aditya Wardhana, the Executive Director of the Indonesian AIDS Coalition (IAC). This is the motto that he lives by, a motto that drives the work of IAC and how communities and civil society are meaningfully engaged in the HIV response in Indonesia.
IAC is a community-led organization based in Jakarta and was recently appointed the second community Principal Recipient to implement the Global Fund to Fight AIDS, Tuberculosis and Malaria’s (Global Fund) grant for HIV in Indonesia for 2022–2023—a feat, since only a handful of community-based organizations nationally or regionally hold Global Fund Principal Recipient status.
“Often, communities are seen as beneficiaries of programmes or as patients, not as decision makers. The IAC has always strived to shake up this dynamic. We believe that being a Principal Recipient will give us greater control over the issues that impact our communities and will set the direction of the national HIV response that puts communities at the centre of it,” explained Mr Wardhana.
In Indonesia, there are still significant gaps in the HIV response. Treatment coverage is low, with only 26% of people living with HIV on treatment, prevention is still lagging and stigma and discrimination remains high. IAC has identified three priorities to improve the HIV response in Indonesia, which include recognizing community health workers as health workers, creating more sustainable financing to reduce reliance on external donors and reforming laws and policies that discriminate and lack redress mechanism for victims of discrimination.
Networks of people living with HIV deliver life-changing services to those most affected and provide support for adherence to treatment, prevention and other essential health services. The involvement of civil society has been crucial in successfully advocating for sustainable financial resources, improving HIV programming and advancing human rights.
Over the next couple of years, IAC will work on these priority issues with the support of civil society organizations, United Nations partners and other stakeholders. IAC will continue to manage the human rights and community system strengthening programme, supported by the Global Fund and the Ministry of Health. Community system strengthening and community-led monitoring are integral parts of the HIV response. The programme ensures that community-based organizations play an active role in monitoring access to services, community programme quality assurance and human rights violations.
Since the organization’s foundation, the UNAIDS Country Office for Indonesia has been an ally and key partner, supporting IAC throughout the Principal Recipient selection process. “We know how important the role of communities is at all levels of the HIV response. We will continue to support IAC by providing technical assistance and capacity-building, working in collaboration to promote the meaningful engagement of communities and civil society in the HIV response,” said Krittayawan Boonto, the UNAIDS Country Director for Indonesia.
IAC, with support from the United Nations Population Fund in Indonesia, will soon establish a peer-led HIV prevention programme for female sex workers, offering differentiated service delivery to increase the uptake of HIV prevention services. Through the programme, they will also empower communities through capacity-building initiatives to drive the greater involvement of civil society in decision-making, especially in forming policies that directly impact the health and well-being of communities and vulnerable populations. Moreover, IAC plans to integrate gender-based violence screening into its outreach programmes. A human rights-based approach is essential to ending AIDS as a public health threat. This approach will create an enabling environment for successful HIV responses and affirms the dignity of people living with or vulnerable to HIV.
IAC will be responsible for managing US$ 17 million to implement the above programmes, with eight organizations across Indonesia as subrecipients.
“We will dive deep into these challenges and hopefully change the landscape of the HIV response. We believe that a more participatory approach will re-energize communities and remind them why HIV is still important and how programmes designed by communities for communities can save lives. This is what we will work towards; this is how we will end AIDS by 2030,” said Mr Wardhana.
Our work
Region/country



Feature Story
An HIV vaccine: who needs it?
21 July 2021
21 July 2021 21 July 2021The participants of the International AIDS Society (IAS) Conference on HIV Science session on an HIV vaccine were welcomed by Lucy Stackpool-Moore, Director, HIV Programmes and Advocacy at the International AIDS Society, after which Susan Buchbinder, from the University of California, San Francisco, and the San Francisco Department of Public Health, made introductory remarks. Two recorded presentations were then shown, by Kevin De Cock and Gabriela Gomez, speaking, respectively, on the need for and role of an HIV vaccine and on modelling science around the requirements and impact of a putative vaccine.
UNAIDS’ Science Adviser, Peter Godfrey-Faussett, then moderated a lively panel discussion that included Yazdan Yazdanpanah, Kundai Chinyenze, Rachel Baggaley, Daisy Ouya, Jerome Singh and Paul Stoffels.
The first question was on whether a vaccine for HIV, if it arrived, would be too late in view of the other HIV prevention modalities available. The consensus was that a vaccine is still needed, especially in low- and middle-income countries and for key populations. The participants then discussed how good a vaccine would need to be. Relevant issues include efficacy and durability, but a priority is proof of concept of activity. The participants acknowledged that initial inconvenient dosing schedules are justified if it can be shown that a product is protective. Minimum efficacy probably needs to be in the region of 50–60% for products to be taken forward.
The discussion also covered engagement by big pharma—Johnson & Johnson is currently the major company pursuing HIV vaccine research, in conjunction with diverse governmental, nongovernmental and clinical partners. It was emphasized that people and individual motivations drive the science, both for HIV prevention and treatment.
Inevitably, the comparison of vaccine development for COVID-19 and HIV came up. The panellists emphasized, however, that the reasons for a lack of success so far in HIV was largely related to the complex nature of HIV itself.
The discussion ended on a note of realistic optimism, with acknowledgment of the benefits of scientific investment in HIV vaccine research to date, including for COVID-19, but with recognition that long-term commitment is still required. The results of the two ongoing phase three trials (Imbokodo and Mosaico) are eagerly awaited.
Quotes
“A vaccine would not be too late; it would be key to getting back on track.”
“For a comparison group in a phase three trial, the “standard of prevention” is a key question.”
“A world without HIV needs a vaccine.”
“We need advocacy for vaccine research in a changing prevention landscape.”
Related



Feature Story
2025 AIDS targets: the next generation of goals for the global AIDS response
21 July 2021
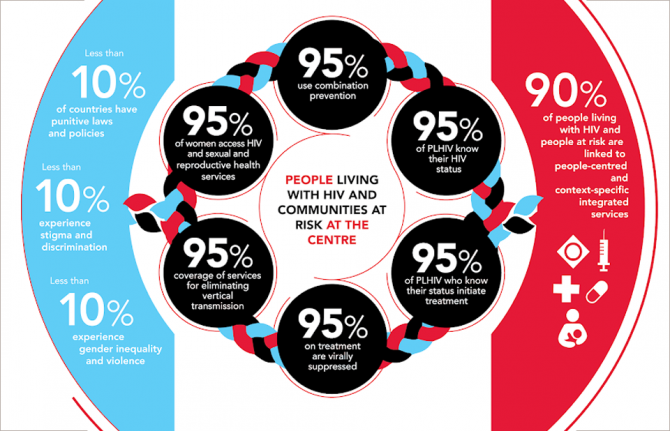
21 July 2021 21 July 2021At a session at the International AIDS Society (IAS) Conference on HIV Science, the participants discussed the new AIDS targets for 2025, which are included in the UNAIDS Global AIDS Strategy 2021–2026 and the 2021 United Nations Political Declaration on AIDS.
The session aimed to make the 2025 targets known more widely among the attendees of the conference. The panel was moderated by Luisa Frescura and introduced by Shannon Hader, the UNAIDS Deputy Executive Director of Programmes. The panel included Adele Benzaken, the Co-Chair of the target-setting process, Aleny Couto, Mandisa Dukashe, Birgit Poniatowski, Erik Lamontagne, Peter Ghys and José A. Izazola.
The different targets, including targets for services, integration and societal enablers, were discussed, framed within the Sustainable Development Goals, and the financial resources needed to achieve them in low- and middle-income countries were highlighted.
The global 2025 targets for the AIDS response are more granular than the targets for 2020. They recognize that societal, service and system enablers are needed to reach the high levels of service coverage and impact needed, while emphasizing the importance of integrating the HIV response to achieve universal health coverage and the Sustainable Development Goals.
The session heard that recommendations for prevention services are given in accordance with the specific needs of populations or groups and their risk of acquiring HIV, with a particular focus given to key populations. The participants also heard that testing and treatment services need to be scaled up in each and every subgroup in order to avoid them being left behind and hidden in the general average of coverage.
The participants noted that the ambitious targets are achievable and clearly show the way to reach a sustainable response to HIV globally.
Quotes
“The new targets for 2025 are indeed more ambitious compared to the ones for 2020; actually, they have to be to inform the design of effective programmes for the future.”
“Because of the lack of progress in the last few years, the resource needs will now peak at US$ 29 billion by 2025 instead of peaking at US$ 26 billion by 2020 and will then decrease. If countries achieve these ambitious targets, a larger number of people will benefit by receiving needed services, and a wider benefit will be achieved as the AIDS epidemic will transit into a controlled phase; the resource needs will stop growing, then start declining”.
“Targets are also needed for HIV science. Having ambitious targets is not contradictory with being realistic. Actually, one aspect supports the other.”
Learn more




Feature Story
Opening session of the IAS Conference on HIV Science
19 July 2021
19 July 2021 19 July 2021The International AIDS Society (IAS) Conference on HIV Science opened on 18 July. The participants were welcomed by Adeeba Kamarulzaman, the Chair of the IAS, and Hendrik Streeck, the local Chair of the conference, who held up UNAIDS as an example of the multisectoral approach that was needed for the response to COVID-19. The opening address was delivered by Angela Merkel, the Chancellor of Germany, which was followed by a panel discussion.
The panel’s speakers drew parallels between the need for global solidarity for COVID-19, especially with regard to access to vaccines, and for HIV, recognizing that both viruses spread regardless of borders and need a global response. They also spoke about the imperative to not let the HIV response be slowed because of the COVID-19 pandemic. Repeated emphasis was made on the bi-directionality of COVID-19 and HIV investments, reminding the audience of the importance of investment in HIV science for developments in COVID-19.
Jens Spahn, Germany’s Federal Minister of Health, accepted that the global response to COVID-19 has been slow but stressed that political decisions had been made to increase global vaccine access, and supply would increase briskly in the coming months. Yvette Raphael, a South African activist living with HIV, recounted her struggle to fight stigma and discrimination relating to HIV, gender and race/ethnicity. She reminded the audience that scientific data relate to real people with human relationships.
Soumya Swaminathan, the Chief Scientist at the World Health Organization, reflected on the priorities of primary health care and universal health coverage. Perhaps the most frequent and strongly felt sentiments concerned the need to combat misinformation and disregard for science. “Follow the science” was a phrase that resonated over the course of the rich discussion.
Quotes
“The multilateral response makes a difference—we have learnt that from HIV.”
“Follow the science, that’s really what he feels very strongly about.”
“As activists, we know how to fight.”
“Everyone has to be part of the solution.”
Learn more
Related
Feature Story
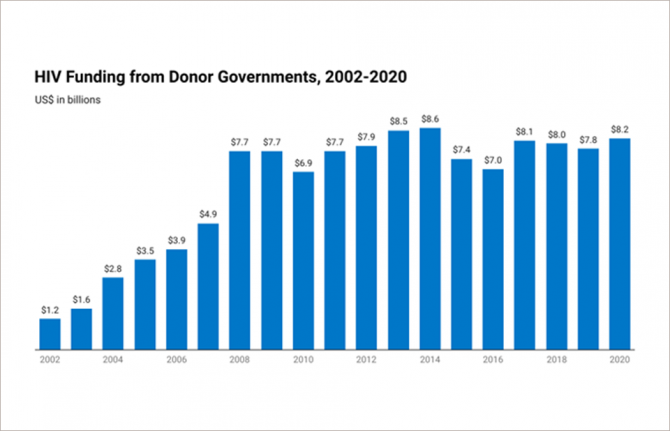
KFF/UNAIDS analysis finds that while donor government spending on HIV increased in 2020, future funding is uncertain with COVID-19 challenges
19 July 2021
19 July 2021 19 July 2021The increase was largely due to disbursement of prior-year multilateral funds. Bilateral funding from donor governments, other than the U.S., continues a downward trend.
A new report from KFF (Kaiser Family Foundation) and the Joint United Nations Programme on HIV/AIDS (UNAIDS) finds that donor government disbursements to combat HIV in low-and middle-income countries increased by US$377 million in 2020, reaching US$8.2 billion in 2020 compared to US$7.8 billion in 2019. Donor government funding supports HIV care and treatment, prevention, and other services in low- and middle-income countries.
The rise in funding is almost entirely the result of an increase in United States contributions to the Global Fund to Fight AIDS, Tuberculosis and Malaria, which was due largely to the disbursement of prior-year funding. U.S. disbursements to the Global Fund are not expected to remain at this level in 2021.
The United States continues to be the largest donor to HIV, accounting for 76% of all donor government funding, followed by the United Kingdom (US$612 million, 7%), Japan (US$258 million, 3%), Germany (US$246 million, 3%), and France (US$216 million, 3%). As other donor governments continue to pull back bilateral funding, the United States accounts for an increasing share of overall funding for HIV from donor governments.
The report reflects prior-year political and funding decisions and does not fully capture the impact of COVID-19 on donor funding decisions.
“While many donor governments are beginning to bounce back from the pandemic, its global impact and related recession make future funding for HIV response unpredictable,” said KFF Senior Vice President Jen Kates. “Not only are some low- and middle-income countries experiencing a ‘third-wave’ of COVID-19, vaccines remain largely out of reach, potentially leading to greater funding needs for HIV and other health services.”
"We are at a critical stage in the AIDS response as countries are confronting the huge challenges posed by the COVID-19 pandemic," said Winnie Byanyima, Executive Director of UNAIDS. "But we do still have an opportunity to end the epidemic by 2030 if donors and countries alike commit to mobilize resources and prioritize health, human rights and equality which are the key components, not only to lead us out of the pandemics of HIV and COVID-19, but they are the cornerstone to economic recovery and security."
These data are included in a broader UNAIDS global report, which examines all sources of funding for HIV relief, including local governments, non-governmental organizations, and the private sector, and compares it to the resources needed to achieve goals related to testing and treatment.
The new report, produced as a long-standing partnership between KFF and UNAIDS for more than 15 years, provides the latest data available on donor government funding based on data provided by governments. It includes their bilateral assistance to low- and middle-income countries and contributions to the Global Fund, UNAIDS, and UNITAID. “Donor government funding” refers to disbursements, or payments, made by donors.
Our work
Partners


Feature Story
UNAIDS saddened by the death of Geoff Makhubo, Executive Mayor of Johannesburg
12 July 2021
12 July 2021 12 July 2021By Mbulawa Mugabe, UNAIDS Country Director for South Africa
It is with great sadness that I received the news that the Executive Mayor of Johannesburg, Geoffrey Makhubo, passed away on 9 July 2021.
Having served in various senior positions in the Johannesburg Council and as the Member of the Mayoral Committee for Finance, Mr Makhubo was appointed Johannesburg Executive Mayor in December 2019, a position that he served with commitment and dedication.
Mr Makhubo was a strong advocate in the response to HIV, and on World AIDS Day 2020 he urged communities to work together to end HIV-related stigma. UNAIDS is grateful for his leadership and commitment to public health and to the HIV response, and for his unwavering support for the Fast-Track cities initiative. Given his commitment to the urban health agenda, Mr Makhubo addressed the global Fast-Track cities conference in 2020 and was a panellist at the United Nations High-Level Meeting on AIDS Fast-Track cities side event in June 2021.
His death is a deep loss for the HIV community and the citizens of Johannesburg.
Mr Makhubo died from COVID-19 complications, following a positive test result in late June.
We extend our sincere condolences to Mr Makhubo’s colleagues, family and friends, and to the city of Johannesburg.
Region/country





Feature Story
UNDP and UNAIDS support more than 300 pregnant and breastfeeding women living with HIV in Abidjan
08 July 2021
08 July 2021 08 July 2021Like the rest of the world, COVID-19 has hit Côte d’Ivoire hard. As soon as the first cases of COVID-19 were confirmed in March 2020, a national response plan was developed by the government. Unfortunately, the restrictive measures to protect the population had an impact on the use of health services, including those related to HIV, threatening the fragile retention in care of people living with HIV. Pregnant and lactating women living with HIV and their children, one of the most vulnerable groups, have been particularly affected, and maintaining their access to services and care was essential to avoid undoing years of effort.
The United Nations Development Programme (UNDP) and UNAIDS joined forces to help retain 333 pregnant and lactating women living with HIV in antenatal, maternity and paediatric services in Abidjan. The project will provide, over nine months, 1000 food kits and 1000 hygiene kits to help beneficiaries with food assistance and help them protect themselves against COVID-19. A food kit contains 20 kg of rice, six litres of oil, 10 pieces of soap and four boxes of children’s flour, and a hygiene kit contains two bottles of hydroalcoholic gel, two bottles of liquid soap and 50 surgical masks. The project also aimed to ensure that the women have access to the comprehensive package of services developed under Côte d’Ivoire’s prevention of mother-to-child transmission of HIV (vertical transmission) programme, to ensure that all exposed children of the project’s beneficiaries are screened early and have access to appropriate care and to document and share good practices.
One of the beneficiaries, Ouattara Maimouna, who has been living with HIV for five years and is a breastfeeding mother of three children, said, “Doctor, this gift was incredibly important to us. It has helped us a lot! This stock of food helps me feed my family. I cannot thank you enough, because I ran out of ways to sustain the small business that used to support my family.”
“About 700 hygiene kits and 700 food kits have been distributed since the project started in December 2020. The United States President’s Emergency Plan for AIDS Relief’s (PEPFAR) implementing partners unanimously indicate that the kits have contributed to the loyalty of pregnant and breastfeeding women to prevention of vertical transmission of HIV and paediatric care services, as well as to self-support groups,” said Brigitte Quenum, the UNAIDS Country Director for Côte d’Ivoire.
At this stage of implementation, some lessons learned are already emerging. The project has been very well received by the beneficiaries because of their vulnerability, which has been aggravated by the COVID-19 crisis. The support has helped to increase their compliance with appointments at the various prenatal consultations, to improve the continuity of treatment and viral load testing for pregnant and breastfeeding women and to strengthen the link between women living with HIV and the staff providing both clinical and community care. The project also emphasizes the importance of taking into account the social component in the care of women in prevention of vertical transmission of HIV services.
The distribution of food and hygiene kits will continue until the end of 2021. Pregnant and breastfeeding women living with HIV have become more vulnerable in the midst of the response to COVID-19 and assistance strategies that respond to their specific sensitivities must be designed. “The mobilization of UNDP, UNAIDS, PEPFAR implementing partners and their nongovernmental organization partners has ensured a coalition of support for advocacy and the scaling up of outreach efforts to vulnerable populations,” added Ms Quenum. “While this one-time initiative is useful, efforts should be made to integrate other activities, such as nutrition promotion and the integration of a social component in the care of women living with HIV in vertical transmission services and other care sites.”
An HIV-sensitive and inclusive social protection assessment will start in the coming months in collaboration with the key ministries involved. Mobilization of funds for social aspects related to women living with HIV and advocacy for sustainable support measures will be required.
Region/country
Related




Feature Story
African first lady technical advisers to align OAFLAD’s strategic plan with the new HIV targets
08 July 2021
08 July 2021 08 July 2021In a briefing co-hosted by the Organisation of African First Ladies for Development (OAFLAD) and UNAIDS, technical advisers to the first ladies renewed their commitment to the HIV response in Africa. Capitalizing on the convening, leadership and advocacy role of African first ladies, they highlighted the need to align national and regional efforts to the new Global AIDS Strategy 2021–2026: End Inequalities, End AIDS and the targets in the 2021 United Nations Political Declaration on HIV and AIDS: Ending Inequalities and Getting on Track to End AIDS by 2030.
The briefing focused on presenting the outcomes of the United Nations High-Level Meeting on AIDS, including the Political Declaration on AIDS, the Global AIDS Strategy 2021–2026 and its new targets, the Education Plus initiative and the Common Africa Position on the High-Level Meeting on AIDS. It highlighted the unfinished business of the HIV response and the continued efforts to meet prevention and treatment targets and adopt a rights-based approach that leaves no one behind.
In her welcoming remarks, Berthilde Gahongayire, the UNAIDS Country Director for Ethiopia and the Director, a.i., of the UNAIDS Liaison Office to the African Union and the United Nations Economic Commission for Africa, reiterated the instrumental role played by African first ladies in putting previous United Nations political commitments into action. She also extended appreciation to the first ladies, who continued to invest in the HIV response during the COVID-19 pandemic in Africa. “We appreciate the support by first lady offices during the COVID-19 emergency in providing socioeconomic support to those vulnerable and marginalized, including protecting services for people living with HIV,” she said.
The technical advisers expressed interest in participating in the Education Plus initiative and integrating the new political declaration targets in their national plans and in the OAFLAD 2019– 2023 strategic plan. Namibia, which was a co-facilitator of the High-Level Meeting on AIDS, shared information on the political declaration and called on the technical advisers to be champions for ending AIDS as a public health threat by 2030.
“I call on all technical advisers to support the popularization, dissemination and alignment of the political declaration and the global AIDS strategy in national programmes,” said Steven Bernardus Harageib, the Technical Director of the Office of the First Lady of Namibia. He added that Namibia is committed to demonstrating leadership in accelerating the AIDS response in Africa.
Moustapha Zakari, from the African Union Commission, on behalf of Margaret Agama-Anyetei, the acting Director of Health, Humanitarian Affairs and Social Development for the African Union Commission, commended the OAFLAD leadership on building momentum after the High-Level Meeting on AIDS. He saluted the commitment of member states in advancing the HIV response through the adoption of a Common Africa Position on the High-Level Meeting on AIDS, which was instrumental in the negotiation of the continent’s priorities in the new political declaration.
The meeting, which was chaired by Michel Mongo from Congo, was attended by more than 30 technical advisers. Mr Mongo closed the meeting by requesting support from UNAIDS to update strategic plans and to articulate the new targets at the country level.

Feature Story
Report shows big COVID-19-related HIV prevention programme service disruptions, but highlights that HIV service innovations and adaptations are possible
01 July 2021
01 July 2021 01 July 2021The COVID-19 pandemic is threatening decades of hard-won development and public health gains. UNAIDS is committed to playing a pivotal role in ensuring that people living with and affected by HIV have the information and support they need during the COVID-19 pandemic and is promoting the development and support measures needed to ensure that access to HIV prevention and treatment services continues uninterrupted.
Launched in 2017, the Global HIV Prevention Coalition aims to bring fresh momentum and clarity to HIV prevention programmes, focusing on 28 countries carrying the highest burden of the HIV epidemic. The Global HIV Prevention Coalition has published a new report, Preventing HIV infections at the time of a new pandemic: a synthesis report on programme disruptions and adaptations during the COVID-19 pandemic in 2020, which provides a synthesis of the status of HIV prevention programming during the COVID-19 pandemic, identifies critical vulnerabilities, risks and major service disruptions and documents responses in a range of settings. The report places a significant focus on gathering information on programme innovations at the community level.
“The COVID-19 pandemic risks reversing the hard-won gains made in HIV prevention, including the 23% reduction in new infections since 2010. And this is at a time when much more still needs to be done to drastically reduce new HIV infections. Gaps and threats to progress show great inequalities, and HIV prevention services and societal barriers for the people most left behind, such as key populations and adolescent girls and young women, have been disproportionately impacted by COVID-19,” said Shannon Hader, the UNAIDS Deputy Executive Director for Programmes.
Inevitably, significant disruptions on HIV prevention services have been observed, and supply chains for crucial HIV prevention commodities, including condoms, lubricants and antiretroviral and other medicines, have been stretched. The report reflects on the early dips observed in the monthly numbers of people served by critical HIV prevention programmes, including huge drops in the number of voluntary medical male circumcisions performed compared to previous corresponding months.
At the same time, while it has vividly exposed and widened inequalities and health inequities, COVID-19 has also shown how to make health systems and other public institutions fairer, more inclusive and better able to meet the challenges of ending the AIDS epidemic. Health-service providers and community organizations have responded to the crisis by changing how they provide HIV prevention services and minimizing disruptions of essential services.
The report highlights COVID-19 impact mitigation innovations and adaptations of HIV services, including multimonth dispensing of condoms, lubricants, needles, syringes and pre-exposure prophylaxis (PrEP), differentiated service delivery and self-testing approaches, alternative access points for prevention commodities such as condoms and PrEP, take-home dosages of opioid substitution therapy for people who inject drugs, the safe continuation of outreach services for key populations and adolescent girls and young women and virtual platforms for prevention interventions—and calls for their scale-up even beyond the COVID-19 pandemic. The report further highlights how the COVID-19 pandemic response has drawn from HIV experts and communities and has taken early decisive action to address critical vulnerabilities, maintain health services and build synergies between the colliding pandemics.
“In over 30 years of developing effective prevention approaches, we have gained substantial knowledge and experience that decision-makers and health programme implementers can use in low- and middle-income countries to make the best possible choices in preventing SARS-CoV-2,” said Dr Hader. “The most pressing needs we hear from communities are the protection of livelihoods: how do people eat, live, care for themselves and survive COVID-19. UNAIDS can help broker services for people,” she added.
The report will support all stakeholders in their preparation of Global Fund to Fight AIDS, Tuberculosis and Malaria COVID-19 Response Mechanism applications, ensuring that proposal writing teams identify key HIV prevention innovations and adaptations that could be supported and scaled-up to regain global HIV prevention momentum and mitigate the impact of the COVID-19 pandemic on HIV services.