




Feature Story
Vibrant civil society remains at heart of the HIV response in Kenya
29 May 2018
29 May 2018 29 May 2018Civil society has played an important role in the response to HIV since the very beginning of the epidemic, calling for access to life-saving medicines, demanding the rights of people living with and affected by HIV and providing critical HIV prevention, care and support. Without civil society, fewer HIV services would be available, particularly to marginalized populations and to people in remote areas.
On a recent visit to Kenya, the Executive Director of UNAIDS, Michel Sidibé, met with members of civil society organizations in Kenya to talk about how to support, reinforce and expand the contribution of civil society towards ending the AIDS epidemic.
“We need a new narrative, not only about HIV treatment but how to restore people’s dignity,” said Mr Sidibé. “We need to demonstrate that no one can better deliver on universal health care than civil society organizations.”
Community responses to HIV result in better health, foster community resilience and are cost-effective. Civil society also needs to be fully involved in decision-making processes to help its work in ensuring respect for human rights, achieving gender equality and diversity and ensuring that no one is left behind.
Wanjiru Mukoma, the Executive Director of Liverpool VCT Health, a Kenyan civil society organization that provides HIV prevention, testing, care and treatment services, facilitated the meeting. She said, “We are at the point where we must frame the HIV agenda. The HIV response cannot be effective without a vibrant civil society.”
The participants asserted that the focus must shift from building the capacity of civil society to meaningful investment in existing capacity in order to increase the impact of its work in the AIDS response.
“Civil society organizations have done a lot of work, but credit does not go to us. We need support to document our work and build our capacity to establish robust monitoring systems of our contribution to Fast-Track,” said Dorothy Onyango, the Executive Director of Women Fighting AIDS in Kenya.
Ensuring the meaningful participation of young people in civil society spaces was also stressed. “We do not want the young at heart to represent us; we are asking for spaces to represent ourselves. We have capacity,” said Joyce Amondi, a young person at the meeting.
During the day, Mr Sidibé also met with Sahle-Work Zewde, the Director-General of the United Nations Office at Nairobi, to discuss sustainability planning to maintain and accelerate the remarkable results that Kenya has achieved towards achieving the 90–90–90 targets, whereby, by 2020, 90% of people living with HIV know their HIV status, 90% of people who know their HIV-positive status are accessing treatment and 90% of people on treatment have suppressed viral loads. They agreed that decentralizing service delivery systems, cutting user fees and stopping the use of falsified medicines would be transformative for the AIDS response in Kenya.
UNAIDS is committed to the meaningful and inclusive participation of civil society at all levels of the AIDS response. By integrating community responses into national AIDS plans and Global Fund to Fight AIDS, Tuberculosis and Malaria concept notes, including budget allocations, UNAIDS supports the funding, development, implementation and monitoring of community service delivery programmes, civil society organizations, advocacy organizations and community networks.
UNAIDS brings civil society organizations together with governments and donors to develop plans, strategies and programmes, review legal and policy environments and respond to emergency and human rights issues. UNAIDS supports civil society organizations to engage in the AIDS response in a coordinated way that respects diverse voices and actions, facilitating civil society advocacy and community-based service delivery.
Region/country
Related





Feature Story
Shining a light on gender-based violence in Kenya: why we must do more
29 May 2018
29 May 2018 29 May 2018Gender-based violence is one of the most persistent violations of human rights across the globe. According to the World Health Organization, about one third of women worldwide have experienced violence. Intimate partner violence increases the risk of HIV, in some regions by up to 1.5 times. Among marginalized populations, a high prevalence of violence is linked with higher rates of HIV infection, in particular among transgender women.
In Kenya, a recent study found that 32% of young women aged 18–24 years and 18% of their male counterparts reported experiencing sexual violence before the age of 18. Gender-based violence reduces the bargaining power to negotiate safer sex, stay on treatment or remain in school.
To shine a light and galvanize action to end gender-based violence in Kenya, the United Nations Population Fund (UNFPA), together with the Kenya Medical Women’s Association and the Kenya Women Judges Association, and partners, launched the Tuongee (Let’s Talk) Campaign on 25 May at an event hosted by Nicolas Nihon, the Ambassador of Belgium to Kenya and UNFPA.
Speaking at the launch, Michel Sidibé, the Executive Director of UNAIDS, said, “Gender-based violence and HIV are intertwined epidemics. If we are to transform either, we must address the structural barriers that drive both.” He spoke about the need to equip young women with the skills and capacities to make informed decisions about their health and underscored the critical importance of engaging boys and men early to change behaviours and challenge norms that allow gender-based violence to persist.
A young survivor of gender-based violence from Kisumu, a port city on Lake Victoria, made a moving and powerful testimony, reminding participants of the critical importance of the campaign and the need to speak up to help survivors to accept and heal. She also urged parents to talk to their children about violence and to support them in speaking out.
Mr Nihon underlined the commitment of the Government of Belgium to combat all forms of gender-based violence and commended the work of the Kenya partners in supporting the survivors.
“Gender-based violence is, unfortunately, not an uncommon phenomenon against women and girls,” said Ademola Olajide, UNFPA Representative to Kenya. “Care and support for the survivors is critical to eliminate gender-based violence and requires a multisectorial approach.”
The participants affirmed that community-level action combined with global advocacy and structural change can lead to change and that there is much potential to build on the good work already done to accelerate results.
Achieving gender equality, advancing women’s empowerment and fulfilling the sexual and reproductive health and rights of women and girls are central to UNAIDS’ work and crucial to reaching the Sustainable Development Goals and achieving the targets set in the 2016 United Nations Political Declaration on Ending AIDS.
UNAIDS, together with a wide range of partners, including women living with HIV and women’s organizations, are working to ensure that women and girls everywhere have their rights fulfilled and are empowered to protect themselves against HIV and that all women and girls living with HIV have immediate access to HIV treatment and care.
Related




Feature Story
First Lady of Kenya champions a generation born free from HIV
06 June 2018
06 June 2018 06 June 2018Margaret Kenyatta, the First Lady of Kenya, reinforced her commitment to champion the elimination of mother-to-child transmission of HIV in a meeting with UNAIDS Deputy Executive Director Gunilla Carlsson in Nairobi, Kenya, on 29 May.
The First Lady and Ms Carlsson discussed the Beyond Zero platform, a groundbreaking initiative spearheaded by the First Lady. Through Beyond Zero, the First Lady has mobilized resources from the private sector to respond to the health and well-being of women and children, with a focus on HIV and sexual and reproductive health.
“There is so much momentum and support from Kenyans themselves for the Beyond Zero initiative. They feel that it is theirs and that they own it,” said Ms Kenyatta.
Beyond Zero has delivered 52 mobile clinics to every county in Kenya. The operationalization of the clinics has resulted in substantial community mobilization and demand creation for HIV services. Initiatives such as Beyond Zero have contributed to significant progress in the AIDS response in Kenya, with new HIV infections among children aged 0 to 14 years reducing from about 14 000 in 2013 to 6100 in 2016, while in the same period the percentage of mothers delivering without a skilled health provider decreased from 56% to 34%.
Building on those gains, the First Lady launched a new framework earlier this year to advance the Beyond Zero initiative. The framework adopts a life-cycle approach, addressing challenges, including HIV, at different stages of life. Ms Kenyatta’s championship for Kenya to reach validation by the World Health Organization for the pre-elimination of mother-to-child transmission of HIV is a core commitment of the framework.
“Beyond Zero is a powerful initiative. An advocacy platform that has fostered public–private partnership for the health agenda and the elimination of mother-to-child transmission of HIV in particular,” said Ms Carlsson.
Related resources
Region/country


Feature Story
Stepping up sexual and reproductive health services in Egypt
04 June 2018
04 June 2018 04 June 2018In response to a call by women living with HIV in Egypt for an increase in the availability of quality sexual and reproductive health services delivered free from stigma and discrimination, UNAIDS mobilized partners and engaged with Egypt’s national AIDS programme.
The result was a pilot project that ran from 2016 to 2018 in which almost 300 women across the country were provided with family planning, antenatal care, support during delivery, postpartum care and guidance on the prevention of mother-to-child transmission of HIV.
On 30 May, national stakeholders, including representatives of the Ministries of Foreign Affairs and Health and Population, civil society, academia and people living with and affected by HIV, gathered to highlight the key achievements, experiences and lessons learned from the pilot.
“I benefited from the project counselling service throughout my pregnancy. I started taking medicine, and, with follow-up, I had a child free from HIV, which I never thought was possible or an option,” said an Egyptian woman living with HIV.
The pilot project achieved outstanding results, reaching nearly double the number of people originally planned to be reached and building institutional expertise in sexual and reproductive health. Counselling and psychosocial support was provided by health professionals and supported by women living with HIV.
“This project is a continuation of the collaboration and fruitful partnership between UNAIDS and the Egyptian Government. We congratulate the Government of Egypt for addressing the needs of a highly marginalized population,” said Ahmed Khamis, the UNAIDS Country Manager for Egypt.
Dr Ahmed Khamis, UNAIDS Country Manager, gives the opening speech on the closing and final dissemination of key results of the “Enhancing Sexual and Reproductive Health of Women Living with HIV” pilot project; with Dr Alaa Eid, Under Secretary for Preventive Medicine, Ministry of Health and Population, H.E. Laurens Westhoff, Ambassador of the Netherlands in Cairo and Ambassador Seif-alla Kandeel, Director of UN Specialized Agencies, Ministry of Foreign Affairs (from left to right). Photo taken by Mohamed Ezz
The pilot programme was funded through financial support from the Embassy of the Netherlands in Egypt and covered the Giza and Gharbia Governates of Egypt and was later extended to the Dakahlia Governate.
“The Netherlands is strongly committed to curbing the spread of HIV worldwide as an integral part of our contribution towards the achievement of the Sustainable Development Goals. We are proud of our partnership with UNAIDS and the Egyptian Ministry of Health. The Netherlands Government is committed to participate in the next step,” said Laurens Westhoff, Ambassador of the Netherlands to Egypt.
As the next step, the Netherlands is finalizing an agreement for a scaled-up three-year project, doubling the number of women living with HIV reached.
“There is no silver bullet to combat HIV. It’s only through partnership that the challenges of awareness, attention and access to medicine can be tackled,” said Seif-Allah Kandeel, Director, United Nations Specialized Agencies, Egyptian Ministry of Foreign Affairs.
Region/country



 and UNAIDS, in collaboration with the World Health Organization and the Fondation Chirac, hosted a conference entitled Ac")


Feature Story
A pledge to respond to falsified and substandard health products in francophone Africa
29 May 2018
29 May 2018 29 May 2018Twenty-five countries and 10 international organizations have pledged to respond to falsified and substandard medicines in French-speaking Africa.
On the sidelines of the 71st session of the World Health Assembly on 22 May, the Organisation internationale de la Francophonie (OIF) and UNAIDS, in collaboration with the World Health Organization and the Fondation Chirac, hosted a conference entitled Access to Quality Medicines and Other Medical Products in Francophone Africa, which brought together nearly 400 participants, including a number of health ministers. They adopted a declaration with commitments to advance access for all, especially the poorest, to assured-quality health products.
Thousands of people die each year because of falsified or substandard medicines, especially in many African countries, where up to seven out of 10 medicines don’t meet the quality standards required by international health regulatory agencies.
“Finding ways and means for better access to quality medicines and medical products in developing countries, especially in Africa, at all costs is now an emergency because, despite conventional international measures, the intensifying scourge of falsified medicines continues to wreak havoc among the poor,” said Patrice Talon, the President of Benin.
Michel Sidibé, the Executive Director of UNAIDS, agreed. He said, “There is an urgent need to support efforts to stop the entry into the market of falsified and substandard medicines everywhere, including African countries. Access to quality medicines is at the heart of the right to health for all and it is also a prerequisite for universal health coverage.”
The signed declaration aims to foster mechanisms to assure the quality of all health products that reach the African market. Therefore, it calls for the strengthening of health regulatory capacities in the continent, paving the road for the local production of medicines.
OIF’s Secretary-General, Michaëlle Jean, would like the document to be the basis of an action plan. “We intend to raise this with all heads of state and government of the francophone area at the 17th Francophonie Summit in October, mobilizing them around concrete solutions and sustainable financing at the national, regional and international levels,” she said.
Related links



Feature Story
African parliamentarians consider historic resolution on advancing the right to health
14 May 2018
14 May 2018 14 May 2018Parliamentarians from across Africa are considering a historic resolution to promote the right to health and achieve targets on HIV, tuberculosis, malaria and other health emergencies, such as cervical cancer and hepatitis.
Michel Sidibé, the UNAIDS Executive Director, addressed the Pan African Parliament on 9 May to urge its members to express their firm commitment and determination to end the AIDS epidemic and deliver on the Abuja Declaration and the plan of action on achieving health targets in Africa. The plan of action resulted from a high-level parliamentary meeting convened in October 2017 by UNAIDS in partnership with the Pan African Parliament and the African Union.
“A Pan African Parliament resolution will help to achieve health targets in Africa. Parliamentarians, as champions in their communities, can help achieve these targets,” said Mr Sidibé.
The final decision of the parliament will be confirmed after the sixth ordinary session of the fourth parliament concludes on 18 May. The resolution will be the first of its kind for the Pan African Parliament since it commenced in 2004.
“AIDS is not over. We need to reach everyone who does not yet know that they are HIV-positive,” said Kgalema Motlanthe, former President of South Africa.



Feature Story
Global HIV Prevention Coalition accelerates action to reduce new HIV infections
23 May 2018
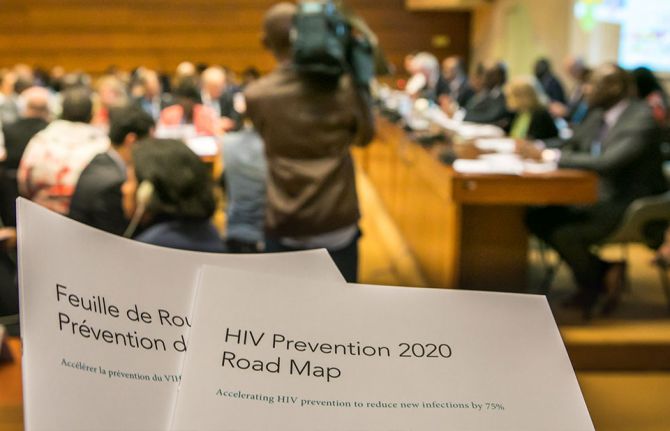
23 May 2018 23 May 2018The Global HIV Prevention Coalition has launched its first progress report.
Taking stock of the progress made in strengthening political commitment for HIV prevention and reducing new HIV infections, the report shows that significant progress has been made since the launch of the Global HIV Prevention Coalition six months ago. National prevention coalitions have been established to accelerate and better coordinate responses, new and ambitious prevention programme targets have been set in many countries and HIV strategies that focus on prevention have been launched.
“There are many promising country examples across the coalition we can learn from,” said Sicily Kariuki, the Minister of Health of Kenya.
Good programme examples highlighted at the event include strong condom programmes in some southern African countries and high voluntary medical male circumcision coverage in several eastern African countries. Strong programmes for key populations, including in India and Ukraine, and pre-exposure prophylaxis being rapidly introduced and expanded in Brazil and Mexico, as well as in South Africa and Kenya, were also noted.
However, the progress report also shows that much still needs to be done. Policies on age of consent continue to represent major barriers to adolescents accessing services. Punitive laws and law enforcement practices hinder access by key populations.
“Every day, there are 1000 new HIV infections among young women and adolescent girls. Prevention programme gaps remain huge,” said Michel Sidibé, the Executive Director of UNAIDS.
For prevention efforts to be sustainable, civil society should be meaningfully engaged in all national prevention coalitions, and their expertise and comparative advantage in implementation used. HIV prevention also needs to be adequately funded.
“Four main reasons that were holding us back were identified when we formed the coalition: gaps in political leadership, policy barriers to effective prevention, gaps in prevention financing and lack of systematic programme implementation at scale. With the adoption of the Global Prevention 2020 Road Map we committed ourselves to address these issues,” said David Parirenyatwa, the Minister of Health and Child Care of Zimbabwe.
More than 200 delegates, including 11 ministers of health from coalition countries, as well as ministers from three additional countries that newly joined the coalition—Botswana, the Islamic Republic of Iran and Myanmar—attended the launch event, held on 22 May at the 71st World Health Assembly in Geneva, Switzerland.



Feature Story
HIV transmission filmed live by French scientists
28 May 2018
28 May 2018 28 May 2018A team of French researchers has succeeded in filming HIV infecting a healthy cell. UNAIDS spoke to Morgane Bomsel, Research Team Director at the French National Center for Scientific Research (CNRS), about the feat.
What motivated you to film HIV transmission?
Morgane Bomsel: HIV transmission has not been studied much and we had no precise idea of the exact sequence of events leading to HIV infection of genital fluids during sexual intercourse. Neither did we know how immune cells are infected and what the consequences are. The vast majority of new HIV infections are acquired via the genital and rectal mucosa; however, the outer layer, the epithelium, of those tissues varies and affects how HIV enters the body.
What were the challenges?
MB: The challenges involved building an experimental model that mimicked genital mucosa infected by genital fluids suitable for live imaging. We reconstructed in vitro human male urethral mucosa based on human cells, the surface of which had been engineered to be red, and an infected white blood cell (a T lymphocyte, the main infectious element in sexual fluids) that was engineered to be fluorescent green and in turn would produce fluorescent green HIV infectious particles.
We had to render the system fluorescent to be able to visualize it and track HIV entry in the mucosa by live fluorescent scanning. Finally, we had to devise a system to allow the microscope lens to visualize the contact between the cells. All of this, of course, was done in an extremely secure setting and all of us were wearing two pairs of gloves and a hat, a coat, glasses and a mask.
When did you know you had a breakthrough?
MB: Our eureka moment was when we captured on film the spillage of a string of viruses, like a gun showering bullets. This lasts for a couple of hours and then, as if the infected cell has lost interest, it detaches itself and moves on.
Please walk us through the video
MB: The HIV-infected cells are labelled in green and produce fluorescent viruses that appear as green dots.
What we see is the HIV-infected cell attaching itself closely to the outer layer, the epithelium, of healthy reconstructed cells of a genital tract mucosal lining.
White blood cells of the immune system, macrophages, that usually engulf foreign substances, debris or cancer cells are seen engulfing the red particles slightly moving next to the blue macrophage nucleus.
The HIV-infected cell approaches the surface of the mucosa and places itself gently on the surface. Owing to, or induced by, contact, the infected cell recruits preformed viruses towards the cell contact (the intense yellow green patches) and then starts to spit those preformed viruses as full infectious viruses that appear as green dots.
These green viruses penetrate the outer layer of the tissue by a process called transcytosis—a type of transcellular transportation. The viruses enter the cell and exit, still infectious, at the other side of the epithelial barrier. As a result, HIV penetrates the types of white blood cells responsible for detecting, engulfing and destroying foreign substances and infects them. Once inside the nucleus, the virus inserts itself in the genetic material, the DNA, and the blood cells that are meant to protect the body start to produce viruses.
Interestingly enough, the video showed that the production of viruses does not last very long. After three weeks, the infected white blood cells become dormant and a reservoir of white blood cells is formed.
What makes HIV particularly tricky to cure?
MB: Attempts to cure HIV have been very difficult because of the dormant infected white blood cells. Those cells are hard for the immune system to find and kill, and for the scientist to study. Antiretroviral medicines prevent the virus from spreading throughout the body and the immune system targets cells that are actively transcribing viral DNA. But because of the reservoir, these cells become a problem if a patient stops taking antiretroviral therapy. They can slowly awaken, allowing the virus to replicate freely.
Related links



Feature Story
Civil society builds a coalition to accelerate results in western and central Africa
15 May 2018
15 May 2018 15 May 2018Western and central Africa has faced many challenges, from conflicts and humanitarian crises to political instability and the devastating Ebola epidemics. At a time when the global response to HIV is accelerating, millions of people in the region are being left behind. Globally in 2016, 70% of all people living with HIV knew their HIV status, 53% of all people living with HIV were accessing treatment and 44% of all people living with HIV were virally suppressed. In contrast, the western and central African region lags behind, achieving only 42%, 35% and 25%, respectively, in 2016. The gap is considerable in that region: 4.0 million people living with HIV are not receiving treatment and 310 000 adults and children died from AIDS-related illnesses in 2016.
In order to share experiences, challenges and information on successful programmes, representatives of civil society organizations involved in the AIDS responses across western and central Africa gathered in Somone, Senegal, from 7 to 10 May. Technical and financial partners also took part in the discussions.
“Eighty civil society leaders from 17 countries in western and central Africa are eager to take up a central role in the implementation of the western and central Africa catch-up plan as actors of social change and political transformation,” said Patrick Brenny, the Director of the UNAIDS Regional Support Team for Western and Central Africa.
The participants developed innovative solutions to overcome barriers to national AIDS responses and to improve the unity and collaboration of local civil society organizations. They examined progress and setbacks in the implementation of national catch-up plans and shared experiences of violations of human rights related to HIV status and stigma and discrimination.
Consensus emerged that efforts should be focused on bridging the gaps in paediatric care and treatment, in particular in the context of the lack of social protection schemes for orphans and other children made vulnerable by AIDS. The region has seen a worrying trend in increasing mortality among adolescents living with HIV. Lack of access to comprehensive sexuality education, a high age of consent to access sexual and reproductive health information, services and treatment without parental agreement and taboos around youth sexuality were raised as some of the obstacles to be overcome.
Successful innovations and programmes with key populations and other vulnerable groups were shared. There was wide consensus about the role of community health systems to reach remote populations and vulnerable groups, while protecting confidentiality.
“It is high time that we increase investments to guarantee access to antiretroviral medicines, have better paediatric medicines, implement family testing approaches and scale up social protection programmes to protect all vulnerable mothers and children,” said Christine Kafando, Coordinator of the Hope for Tomorrow Association in Burkina Faso.
The participants will build on the progress made by organizing national dialogues around the catch-up plan for the region. The development of a regional platform for advocacy and technical support will be further discussed to enable stronger and more resilient civil society to play roles in national AIDS responses and other global health challenges.
“Each stakeholder gathered here plays a central role in their respective national AIDS response. Each brings invaluable experience to the table. We need to build on this energy to renew our commitment to work together for much needed breakthroughs for the region to bring HIV under control,” said Daouda Diouf, the Executive Director of ENDA Santé in Senegal.


Feature Story
Artificial intelligence not necessarily beneficial for LGBTI community
21 May 2018
21 May 2018 21 May 2018One of the most watched events of the year got Cynthia Weber wondering: can the use by Sky News of artificial intelligence (AI) at the wedding of Prince Harry and Meghan Markle be a good thing?
For the first time in history, a news broadcaster used AI facial recognition technology during a live broadcast. Cynthia, a professor of international relations and gender studies at the University of Sussex, explained that using software to name wedding guests may be a nifty trick, but there are worries about the implications.
“Some claim that this technology can identify a person’s sexual orientation,” Cynthia said while speaking during an event for the International Day against Homophobia, Transphobia and Biphobia in Geneva at UNAIDS headquarters.
Referring to a Stanford University study that analysed more than 35 000 images on a United States dating website of white, able-bodied, 18–40-year-olds, the researchers compared their AI-generated sexual orientations against sexual orientations researchers found in dating profiles. The study claimed that AI facial recognition technology could determine a person’s sexual orientation with up to a 30% greater accuracy than people can.
Cynthia said that LGBTI advocacy organizations labelled the study junk science—the study used a skewed sampling in terms of race and age and the study equates sexual orientation with sexual activity. “The result is that the study’s artificial intelligence algorithm only finds what it was programmed to find: stereotypes about straights, gays and lesbians,” said Cynthia.
Cynthia believes that AI knowledge may generate opportunities in many fields, but sees far more risks and dangers than advantages for LGBTI people.
When AI meets facial recognition technology and a sexual orientation algorithm, at least four issues arise. First, privacy. In national and international law, a person’s face is not protected by privacy laws. That allows faces to be scanned and read by everyone, from governments to Sky News.
Secondly, accuracy. “In a world beyond the royal wedding, artificial intelligence facial recognition technology is far from perfect, even when it just tries to match names with faces, much less when it tries to match presumed sexual orientations with faces,” Cynthia said.
For Cynthia, the key issue is knowledge. How does a sexual orientation algorithm know better than an individual his or her sexuality? Cynthia considers the binary approach of code and computer-readable data not compatible with the vast gender and sexuality spectrum.
Finally, the issue of what the AI information will be used for worries Cynthia. “Let Sky News use it for wedding commentary, but what if the police use it in countries where homosexuality is outlawed?” Cynthia asked.
For Cynthia, AI and sexual orientation are not necessarily mutually beneficial. Cynthia understands that AI influences imagination and drives innovation, but believes that categorization of people usually introduces more harms than benefits.
Cynthia concluded by saying, “People have to make sure that artificial intelligence is ethically driven, not just technologically driven.”
The event was organized with the Swiss LGBTI Pride@Work association and UN Globe, a United Nations-wide LGBTI organization, and was held on 16 May.

