

Update
World AIDS Day 2019: Speech by UNAIDS Executive Director Winnie Byanyima
01 December 2019
01 December 2019 01 December 2019I am humbled and excited to be with you in Orkney, in the North West Province of South Africa, to commemorate my first World AIDS Day as the UNAIDS Executive Director.
Thank you for the warm welcome from the heart of your community.
On World AIDS Day, and indeed every day, we remember the millions of lives lost to HIV over the past 40 years, more than three and a half million of them here in South Africa—lives lost to despair, stigma and exclusion.
We also celebrate the struggles and resilience of those alive today because of the huge progress the world has made against the epidemic.
I begin by paying tribute to your liberation movement, which started in townships across South Africa. Your struggle inspired and moved the whole world to action to end the evil system of apartheid. Amandla!
Eyes of the world on South Africa
The eyes of the world are again on South Africa.
After starting late, today you are making remarkable progress against AIDS! More than five million South Africans living with HIV are now on antiretroviral therapy—20% of all the people on treatment in the world.
There was a 53% reduction in the number of AIDS-related deaths from 2010 to 2018.
More than 95% of pregnant women living with HIV are on treatment.
HIV incidence declined by 44% between 2012 and 2017. Great progress!
But even here in South Africa, with all this progress, we cannot rest, and we are still on a journey. Almost 2.5 million people living with HIV are not yet on treatment. We have a job to do. There are more than 1400 new HIV infections among adolescent girls and young women every week. This is intolerable.
So today, on World AIDS Day, here in South Africa and around the world, let us commit to overcoming the challenges and barriers we still face.
Governments have committed to ending AIDS by 2030. We must keep this promise. But business as usual will not get us there.
I am going to talk about five things we need to do, faster and in a more focused way, to beat AIDS.
Women and girls paying the highest price
First, we won’t beat AIDS unless we make huge progress on the rights of women and girls and gender equality in Africa.
It is unacceptable that, worldwide, HIV remains the leading cause of death for women aged 15–49 years.
Millions of poor women and girls are denied the right to make decisions about their health and their bodies.
Fifteen million adolescent girls (aged 15 to 19 years) worldwide have experienced forced sex at some point in their life.
Three billion women and girls live in countries where rape within marriage is not a crime.
Enough is enough.
All women and girls must have the right to choose if they have sex, and with whom, and how to protect themselves.
We need to bring power, equality and agency to all young women and girls.
When we know that keeping girls in school reduces their risk of acquiring HIV, we must empower all girls to stay in school.
We must bring the power of movements together, the power of the HIV movement, the youth movement and women’s movements, to fight for gender equality and end gender-based violence—then we will beat AIDS.
Second, we must protect the human rights of all people, end marginalization and the terrible injustice of AIDS-related mortality.
While we should be proud that 24.5 million people around the world are now on life-saving HIV treatment, we cannot accept that 770 000 people died of AIDS-related illnesses in 2018.
We must never accept that in 2019 people living with HIV are still dying of AIDS.
It is not a question of science. It is a question of inequality, powerlessness and exclusion. That, we can change.
The system is finally working for millions of people living with HIV, but it is still failing for those who are marginalized: gay men and other men who have sex with men, transgender people, sex workers, people who use drugs, prisoners, foreign workers, migrants, refugees and people with disabilities.
In 2018, more than half of all new HIV infections were among key populations and their partners.
Social injustices and human rights violations are drivers of HIV. They must be tackled, or we will lose the battle on HIV prevention.
It is everyone’s right to access health and information and to be treated with respect and dignity.
On World AIDS Day, I call upon all countries to repeal laws that discriminate and criminalize groups of people and drive them away from life-saving services.
Third, we need to put the science and technology to work to save lives. The world has spent billions of dollars developing the fastest tests, the best treatment and new prevention technologies, such as pre-exposure prophylaxis (PrEP) and other women-controlled methods.
Now let us put them to work, in every community, in every country.
Here in South Africa, your progress to 90–90–90 is impressive:
- Ninety per cent of South Africans living with HIV know their status.
- Sixty-eight per cent of people who know their status are on HIV treatment.
- Eighty-eight per cent of people on treatment have an undetectable viral load. And we know that undetectable = untransmissable (U = U).
I’d also like to commend progress in some districts here in South Africa that have reached 90–90–90 ahead of the target date.
But what would your first 90 be today if you were not using rapid tests?
What would your second 90 look like if you were still waiting months or years for someone to go on treatment?
How many people would have reached viral suppression if you were still using a treatment regimen of three, or six or 12 pills per day instead of a one-pill fixed dose combination?
In clinics and countries around the world, these outdated tools are what is keeping us from reaching 90–90–90. We cannot end the AIDS epidemic in the twenty-first century using twentieth century tools and approaches.
The true power of science and innovation is only when it is in the hands of the people.
We have only 13 months remaining to reach 90–90–90, and there is so much work to do, so many lives to save.
Today, I am calling on every ministry of health, every national AIDS programme, every community, to be bold and quick to get on the Fast-Track. Let us put science, innovation and technology to work for the people.
Empowered communities accountability
Fourth, communities are the focus of the UNAIDS World AIDS Day report.
On Friday, I visited the Block X clinic in Tshwane and met amazing people living with HIV. I saw how the Ritshizde project, with five leading organizations for people living with HIV, under the leadership of the Treatment Action Campaign, is unleashing the power of community accountability—empowering people living with HIV to monitor the services they access, advocate for changes in how services are delivered and hold officials and service providers accountable.
We can spend billions of dollars or rand, building beautiful clinics to distribute millions of pills. But only if we empower communities at the grass roots to hold service providers accountable and call out injustices will we make a real difference for people.
Here in South Africa, I have learned about Operation Sukhuma Sakhe—this is a model of community development in KwaZulu-Natal that put communities at the centre of development. It is an integrated approach for empowering communities, addressing social drivers and fighting poverty and inequality. I commend the Minister of Health, Zweli Mkhize, for introducing this when he was the Premier of KwaZulu-Natal.
Financing to get to the end of AIDS
Finally, we will not get to the end of AIDS without the resources to sustain the race.
We celebrate the commitment of the Government of South African for committing nearly US$ 2 billion per year from domestic public resources for HIV. South Africa is a trailblazer for investing in the fight against AIDS. I urge all governments to follow its lead.
Yet, Africa, the region with the highest burden, is facing serious financing challenges that undermine its ability to invest in health care for all its people.
There are four particular issues to pay attention to.
The first is international tax avoidance. Billions of dollars of profits are channelled from Africa to tax havens offshore, shrinking the capacity of African governments to invest in health and other vital development priorities.
No one country can solve the problem of corporate tax dodging alone. African countries, which are the biggest losers, must call for urgent, concerted international action. The BEPS 2.0 process promoted by the Group of 20 with the technical assistance of the Organisation for Economic Co-operation and Development is a step in the right direction.
The second issue is the frustrating stagnation and even decline in domestic revenue mobilization across Africa. Despite a decade of economic expansion, progressive tax reforms that could allow for bigger budget allocations for social investments have not happened. African countries lack the systems to capture tax from private investments, especially from international companies. Countries are failing to raise the resources they need.
The third issue is debt. From 2008 to 2017, tax collection to gross domestic product reduced (down from 20% to 18%), while debt stocks grew at a 10% annual rate. While borrowing has allowed African economies to expand, it has now turned into a serious problem.
Half of African low-income countries are already in debt distress or at high risk of being so. Debt repayments are now eating up public budgets, and what we most care for is now under threat: investments in public health, including the AIDS response.
Two examples. In the last three years (between 2015 and 2018), health spending in Kenya dropped by 9% and debt servicing increased by 176%. In Zambia, the figures are even more staggering: there was a nearly 30% drop in health spending and an increase in debt servicing of 790%.
Africa has entered a new debt crisis.
Vulnerable people, including people living with HIV, must not be made to pay the price of the crisis. UNAIDS will work with African countries to chart pathways out of the crisis that protect and increase investments in universal health care, including their AIDS responses.
Fifth and finally, ending AIDS is a shared responsibility. And to the partners and donors here today, I ask you not to roll back at this time of need. The share of aid for public health has stagnated in recent years. This needs to be reversed.
More positively, last month, governments and foundations responded to the call of the President of France, Emmanuel Macron, making unprecedented donations to the replenishment of the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund). This is proof that global solidarity is not exhausted. It is stronger than ever.
We cannot allow the poorest and the most vulnerable to pay with their lives.
I call on all donors, development partners, foundations and the private sector to go the extra mile. Even with the Global Fund replenishment and the amazing support of the United States President’s Emergency Plan for AIDS Relief, we still need to close the growing funding gap to end AIDS once and for all.
Conclusion
Comrades, we can beat AIDS if we focus and work harder and faster towards our 2030 goal.
We must roll back patriarchy and empower women and girls and root out violence against them.
We have to fight stigma, discrimination and criminalization and guarantee the human rights of all marginalized groups.
We must invest in more scientific innovations for prevention, testing, treatment and care and empower communities to lead the response on the ground. We must find national pathways towards sustainable long-term financing of AIDS responses. All these are achievable—they are an exciting and wining agenda!
And when we win, we will not just end AIDS. We will have fairer, more equal and healthier societies.
We will build societies based on gender equality and justice for all.
We will live lives where everyone is valued and can fully exercise their rights and where nobody is left behind.
This is the call of World AIDS Day. This is the call of the 2030 Agenda for Sustainable Development.
The world has only one year and one month left to reach the 2020 targets.
The world has only 11 years to meet its commitment to end the AIDS epidemic and reach the Sustainable Development Goals.
There is no time to lose. We can do it.
Related resources
Printable version
Related



Update
HIV treatment numbers continue to rise
02 December 2019
02 December 2019 02 December 2019For people living with HIV, being on treatment has two advantages: they stay healthy and, if their viral load is suppressed to undetectable levels, they can’t pass on the virus to their sexual partners.
The number of people living with HIV who are on treatment continues to rise, with an estimated 24.5 million on antiretroviral therapy in mid-2019—more than double the number on treatment in 2012. However, treatment scale-up is still not on track to meet the target by the end of 2020 of 30 million people living with HIV on treatment, and with 37.9 million people living with HIV at the end of 2018, the unmet need for treatment is still worryingly large.
Related




Update
Speech by UNAIDS Executive Director Winnie Byanyima at the World AIDS Day 2019 report launch
26 November 2019
26 November 2019 26 November 2019Cabinet Secretary, Acting Governor James Nyoro, colleagues from the United Nations system. Jambo!
Community health volunteers, you are my heroes. I am so happy to be here with you today in Kiambu County, Kenya.
And I thank you for the warm welcome from the heart of your community at the launch of the UNAIDS report, Power to the people.
Thank you, young people. Especially the young person with a disability who just spoke to us, who reminded us that not all people living with HIV are the same—they are all different, and we must be inclusive. We will remember it. We will act on it.
I want to express my sincere condolences and solidarity with the people of West Pokot on the tragic loss of life and property following the torrential rains and landslides. I hurt with you.
Launch of Power to the people
I am here because Africa is the continent still most affected by the HIV epidemic.
More than 25 million people are living with HIV in sub-Saharan Africa—more than two-thirds of the global total of 37.9 million people living with HIV.
I am also here because many countries in Africa are leading the way to end AIDS. We are heroes, fighting the epidemic.
In Kenya, AIDS-related deaths have fallen by more than 50% since 2010, and new HIV infections are down by 30%. This is a great achievement. Great progress in a short time.
Today, I can announce that 24.5 million people living with HIV around the world now have access to life-saving treatment. Great news and great progress.
Joining the marathon to end AIDS
This is a special day for me.
I am launching my first UNAIDS report.
With this new report, I am paying tribute to the families and communities devasted by AIDS, the women’s grass-roots groups and the communities that have mobilized and transformed the AIDS response. I congratulate you. We owe you a lot.
In my country, women got together in villages, bought saucepans and blankets, looked after each other, buried the dead, didn’t let anyone suffer alone. It was the women in our communities who did that.
Today, I am committing UNAIDS to take some big steps in a new direction.
Fight inequality and poverty
The first step is to address inequality and the injustices that fuel the HIV epidemic.
AIDS hurts people who live in poverty. This is a problem for everyone, but a big problem for the poor.
We have to address inequality. It cannot be right that some people get treatment and live long lives, while others cannot access health care and die.
We must fight inequality, lift all people up out of poverty.
We need to provide more services—education, health, social protection. That is how we will end AIDS.
Gender equality and women’s rights are key
We must advance women’s rights if we are to end AIDS, so our second big step in the race to end AIDS must be to tackle gender inequality.
Despite progress in prevention and treatment, HIV remains the leading cause of death for women aged 15–49 years worldwide.
Every week, 6000 young women aged 15–24 years are newly infected with HIV.
Across sub-Saharan Africa, young women and girls face rates of HIV far higher than men and boys.
Young women in sub-Saharan Africa aged 15–24 years are twice as likely to be living with HIV than men of the same age.
These are numbers that shame us all.
This is a gender injustice with tragic repercussions. Why are young women more vulnerable?
If we are going to keep our promises, we must end the gender power imbalances that are driving HIV risk and vulnerability.
We need to champion gender equality and empower young women and girls to transform our societies.
Worldwide, one in three women will experience physical or sexual abuse in her lifetime.
In too many of our communities, a women’s first experience with sex is violent, is forceful. That is the reality.
Yesterday, we launched 16 days of activism against gender-based violence. Every day we should commit to achieve equality for women and girls, so their vulnerability to violence can end.
Here in Kenya, I am concerned about the rate of femicide.
Every week, we read a media report of a woman, often a young woman, killed by her partner.
We need to speak up for these women, call for justice and an end to impunity. The world must be a safe space for all of us.
UNAIDS will pay more attention to fighting those laws, traditions, cultures and practices that enable and perpetuate gender-based violence. A woman’s body is her body.
It is our urgent duty to ensure that all women and girls, of all ages, have unrestricted access to sexual and reproductive health services.
We cannot accept that millions of women still cannot get access to contraceptives, because we know that their right to contraception is core to their empowerment across every aspect of life.
We are doing an injustice to millions of young people who still cannot access the simple health services they need: free condoms, an HIV test without parental consent and pre-exposure prophylaxis.
Keeping girls in school reduces their risk of HIV. We need to ensure that all young people can stay in school, and that every school provides quality comprehensive sexuality education—to know about their bodies, their health.
UNAIDS, together with our Cosponsors—the United Nations Population Fund, the United Nations Entity for Gender Equality and the Empowerment of Women, the United Nations Educational, Scientific and Cultural Organization and the United Nations Children’s Fund—will step up for women and girls, especially in Africa.
Human rights
The third step I ask us to take today is on human rights.
The human rights and citizen rights of women and girls, gay men and other men who have sex with men, transgender people, sex workers, people who use drugs and prisoners are being denied.
Without judgement, we must ensure that they can access HIV services, so this disease can end. We must treat them as equal citizens, so they can enjoy their right to health and get services to protect themselves and their partners from HIV.
One third of key populations do not know their HIV status.
In many countries, we still have laws that criminalize key populations or discriminate against people living with HIV, so they go underground and hide, and when they hide they can’t enjoy their right to health.
The crackdowns and restrictions on gay, bisexual, transgender and intersex groups and campaigns are unacceptable.
Young people are being judged and punished for who they are and who they love.
We will not end AIDS unless we guarantee the human rights of all people, especially key populations.
Funding and resources
Despite progress in recent years, there are still not enough resources available to end the AIDS epidemic. Poor countries are struggling to pay for everything they need—health, education, roads, water, sanitation.
Health should be a top priority. Without healthy people, we will not make progress.
Two-thirds of countries in Africa still charge fees for health care, and millions of people are just one sickness away from falling into extreme poverty.
Despite the world’s commitment to implement universal health coverage, the percentage of people paying catastrophic health costs out of their pocket has only increased in the past five years. Health cannot be a privilege for the rich—it should be a right for everyone.
Public debt has climbed above 50% of gross domestic product in half the countries in sub-Saharan Africa. In a constrained fiscal space, governments must find pathways to a sustainable long-term financing of their HIV responses. We want to work with governments to see how to create fiscal space and manage their priorities within budgets reduced by debt repayments.
During the recent replenishment of the Global Fund to Fight AIDS, Tuberculosis and Malaria, countries and foundations made a historic down payment to advance the end of AIDS. But more work is also needed to ensure that every dollar, euro and shilling is being used effectively.
In many middle-income countries, governments are still paying thousands of dollars more for the same quality medicines that are available to low-income countries for just pennies a day. This is unacceptable. We will try hard to see that prices come down.
Universal access to quality health care is not a commodity—it is a human right.
Conclusion
I do not underestimate the challenges ahead, but I feel a lot of excitement about what can be achieved for people. We are standing on the shoulders of people who fought—how can we fail to finish?
What I have called for today requires some urgent changes.
Changes in how we think what is possible.
Health care for each and every person—this is not impossible.
Changes in how quickly we act.
Changes in how we work as UNAIDS—we need to look at ourselves in the mirror.
But let us be in no doubt, we can end AIDS.
I’ve lost loved ones.
We can go into a future of health for all.
Cabinet Secretary and all the activists here today, I wish you all the best in your endeavours. UNAIDS is right behind you.
Related information
Printable version
Region/country
Related






Update
Women are leading the response to HIV in their communities
25 November 2019
25 November 2019 25 November 2019Juliana Atieno volunteers in her local health facility as a mentor mother, providing advice and support to pregnant women newly diagnosed with HIV. She is also a passionate advocate for survivors of gender-based violence and works to ensure that they receive the support and care they deserve, including by linking them to HIV prevention and treatment services.
Ms Atieno, who is 29 years old and a survivor of gender-based violence, was diagnosed with HIV as a teenager, in 2008, when she was already very ill. She was linked to treatment immediately and today she is healthy and the mother of two young boys, aged two years and nine years, both born free of HIV. Her partner is also HIV-negative. The family lives in the Kiambiu informal settlement, near Nairobi.
On the eve of the launch of UNAIDS’ new report, Power to the people, Ms Atieno told the UNAIDS Executive Director, Winnie Byanyima, how much her work means to her.
“I love my work encouraging young women and girls to get tested for HIV, to take treatment if they need to and to adhere to it so that they can stay healthy and give birth to babies free of HIV,” she says. “I tell them not to worry, that if I made it through, then they can too.”
Women and girls like Ms Atieno are the backbone of care support in their families and communities, providing unpaid and often undervalued work in caring for children, the sick, the elderly and the disabled and underpinning fragile social support systems. The involvement and leadership of women like Ms Atieno is critical in the response to HIV.
“Whenever I meet women like Juliana, I am moved and inspired by their courage and resilience,” said Ms Byanyima. “It’s clear that when women like Juliana have power and agency, real and positive change flows to their families and to their wider communities.”
Ms Byanyima’s meeting with Ms Atieno coincided with the beginning of the 16 days of activism campaign against gender-based violence.




Update
Sex workers often not accessing HIV prevention services
18 November 2019
18 November 2019 18 November 2019Despite the availability of a widening array of effective HIV prevention tools and methods—and a massive scale-up of antiretroviral therapy in recent years—there has been insufficient progress in reducing global new HIV infections, which have fallen by only 16% since 2010.
The United Nations General Assembly’s 2016 Political Declaration on Ending AIDS calls on countries to ensure that 90% of those at risk of HIV infection are reached by comprehensive prevention services by 2020. However, sex workers―and other key populations―often haven’t been accessing the prevention services they need. Country data reported to UNAIDS within the last three years show a widely varying coverage of combination HIV prevention services.
With female sex workers having a 21 times higher relative risk of HIV acquisition compared to the general population, access to suitable HIV prevention options is vital.
Related

 Government ensures continuity of treatment in Malawi
Government ensures continuity of treatment in Malawi
10 February 2025

Update
Statement of commitment to step up action towards ending AIDS, eliminate social injustice and reach the women and girls being left behind
12 November 2019
12 November 2019 12 November 2019This year marks the 25th anniversary of the International Conference on Population and Development (ICPD), where 179 governments adopted a landmark Programme of Action. The Programme of Action unequivocally affirmed reproductive rights as human rights, fundamental to the empowerment of women and girls and to achieving gender equality and sustainable development more broadly.
From 12 to 14 November, the governments of Kenya and Denmark, together with the United Nations Population Fund (UNFPA), are co-convening the Nairobi Summit to mobilize the political will and financial commitments needed to finally and fully implement the Programme of Action.
During the conference, UNAIDS will be reinforcing the importance of HIV prevention, treatment and care as integral to the ICPD agenda. UNAIDS will also be advocating for sexual and reproductive health services for all and access to services that work for and address the needs of adolescent girls and young women.
On the opening day of the conference the Executive Director of UNAIDS Winnie Byanyima made a statement of commitment on behalf of the UNAIDS Secretariat to step up action towards ending AIDS, eliminate social injustice and reach the women and girls being left behind.
I, the Executive Director of UNAIDS, as a co-convenor of the Global HIV Prevention Coalition (GPC), will step it up on the unfinished business of the ICPD Programme of Action, the Beijing Declaration and Platform for Action, and the Political Declaration on HIV and AIDS.
Every week, 6,200 adolescent girls and young women acquire HIV. Maternal mortality is the leading killer of adolescent girls 15 to 19 years old. This is intolerable, unethical, unconscionable—25 years after Cairo.
Despite progress in HIV prevention for adolescent girls and young women, we are leaving too many of them behind, especially those who face intersecting forms of stigma, discrimination and inequality. They face high risks of acquiring HIV and STIs, unwanted pregnancies, unsafe abortions, and being subjected to gender-based violence and harmful practices. This is no surprise; gender norms and taboos about their sexual and reproductive lives and rights are pervasive; access to comprehensive sexuality education remains limited; and the low quality of services restricts choice and falls short of providing young women with the range of interventions they require for their empowerment. The GPC estimates that in 2018, less than half of the areas with high HIV prevalence had dedicated comprehensive HIV prevention programmes—very short of the global target of reaching 90% of adolescent girls and women with these services by 2020.
Meanwhile, we have the know-how to put the power of prevention in their hands and fulfill their rights. We must act urgently to listen to them, to do right by them; and make UHC work for them.
We commend the 28 Ministers from countries with the highest HIV burdens for their political leadership and commitments announced here in Nairobi on 11 November during the GPC Ministerial meeting.
We also heard the calls for action and demands from young women. Our commitment is dedicated to all adolescent girls, and all young people, particularly those from key populations around the world confronted by the HIV epidemic.
UNAIDS commits, at the highest levels, in collaboration with our sister entities of the UNAIDS Joint Programme and wider UN family, to drive decisive political will on HIV prevention and young women’s sexual and reproductive health and rights. Through our collective support to national governments, and with the active participation of civil society and communities of women and young people, in all their diversity, in our decision-making;
Specifically in the African continent, where young women are hardest hit by the epidemic, we commit to pursue a strategic initiative with UNFPA and UN Women to remove the barriers and harmful social norms which result in their higher vulnerability to HIV.
By the end of 2020, the GPC partnership will support countries to:
- Remove parental consent laws for adolescents to access sexual and reproductive health services, including for contraception and HIV testing, prevention and treatment, in 4 countries of sub-Saharan Africa: Lesotho, Malawi, Uganda, and Zambia. Such laws are a threat to public health, and only cause grave harm to young people.
- Ensure access by adolescent girls and young women to integrated sexual and reproductive health information, education and services in areas with extremely high HIV in 7 countries-- Botswana, Eswatini, Lesotho, Mozambique, Namibia, South Africa and Zimbabwe. Emphasis will be on ensuring effective prevention of HIV and STIs within contraceptive services, and expanded contraceptive choice; as well as addressing gender-based and sexual violence as part of intensified, cross-sectoral programmes to unleash social and economic enablers for young women to thrive, and exercise their sexual and reproductive rights.
Globally, we commit to adolescents and young people, and all communities hardest-hit by the HIV epidemic, to:
- Fully leverage the leadership and resources of the Global Fund to Fight AIDS, Malaria and Tuberculosis to best respond to the needs and demands of adolescent girls and young women and other key populations living with or at high risk of HIV, in all their diversity—with emphasis on action for prevention at local and grassroots levels; alongside approaches that tackle poverty, gender discrimination and gender-based violence in their lives.
- Galvanize political will to end social injustice in 30 countries from across regions through the Global Partnership for Action to Eliminate All Forms of HIV-Related Stigma and Discrimination. We must confront head on the fear, threats, violence, persecution, criminal laws, humiliating treatment and violations of the fundamental human rights and freedoms faced everyday by some of the most left behind communities in the world—especially from key populations hard-hit by the HIV epidemic such as sex workers, transgender persons, gay men and other men who have sex with men, other persons of diverse sexual orientations and gender identities, people who use drugs, people in detention, and migrants, among others.
- Finally, the UNAIDS Secretariat will develop and deliver a simplified methodology to assist countries in collecting reliable data on key populations to improve planning and implementation of HIV prevention, treatment and support services, alongside protection of their human rights, safety and dignity—communities so pervasively marginalized and discriminated against that some governments refuse to acknowledge they even exist, much less counted, as rightful citizens of their countries.
Only through the full and swift implementation of these pledges will we ensure the Cairo promises reach everyone on the SDGs road to 2030. And only by putting communities at the centre of our efforts, and investing in community-led, women-led and youth-led responses ---will we be able to deliver a better world for today’s younger generations, and those to come.
The Nairobi Summit on ICPD25

Update
HIV-related discrimination far too high
12 November 2019
12 November 2019 12 November 2019In the early days of the HIV epidemic, pervasive stigma and discrimination against people at higher risk of HIV infection and people living with HIV nearly paralysed the AIDS response. HIV-related discrimination stops people accessing the HIV services they need to stay healthy and can affect incomes and livelihoods and a whole range of other aspects of people’s lives.
Discriminatory attitudes towards people living with HIV remain extremely high in far too many countries. Across 26 countries with recent population-based survey data, the percentage of people aged 15–49 years with discriminatory attitudes towards people living with HIV ranged from 16.9% in South Africa to 80% in Guinea.




, by population group, global, 2018")

Update
Worldwide, more than half of new HIV infections now among key populations and their sexual partners
05 November 2019
05 November 2019 05 November 2019The global distribution of new HIV infections in 2018 crossed a threshold: the majority of global new infections were among key populations and their sexual partners.
This change is a result of the strong progress in settings with high HIV prevalence in eastern and southern Africa, combined with a mixture of progress and setbacks in lower prevalence regions.
Key populations make up a small proportion of the general population, but they are at extremely high risk of acquiring HIV infection. Available data suggest that the risk of HIV acquisition among gay men and other men who have sex with men was 22 times higher in 2018 than it was among all adult men. Similarly, the risk of acquiring HIV for people who inject drugs was 22 times higher than for people who do not inject drugs, 21 times higher for sex workers than adults aged 15–49 years and 12 times higher for transgender women than adults aged 15–49 years.
Learn more
Related



Update
Many prisoners are lacking basic HIV services
28 October 2019
28 October 2019 28 October 2019Environmental, social, cultural, human rights and biological factors all lead to a greatly increased risk of contracting tuberculosis and HIV in prisons.
Risk behaviours such as sharing of used needles and syringes, unprotected sex, sexual violence and lack of access to comprehensive HIV prevention and harm reduction services put people in prisons at heightened risk of HIV and other infections. Globally, HIV prevalence among people in prison is much higher than among the general population, with incarcerated people on average five times more likely to be living with HIV compared with adults outside. Key populations―people who inject drugs, sex workers and, in some countries, transgender people and gay men and other men who have sex men―tend to be overrepresented among incarcerated populations.
Despite the relative ease of reaching people within prisons, HIV services are not provided in prisons in many countries. Across the last three years of country reports to UNAIDS, very few countries reported programme data on the provision of condoms (32 countries), opioid substitution therapy (24 countries) and sterile injecting equipment (three countries) in prisons, but 74 countries reported programme data on antiretroviral therapy coverage and 83 countries reported HIV testing in prisons.
Related
Government ensures continuity of treatment in Malawi
10 February 2025
Update
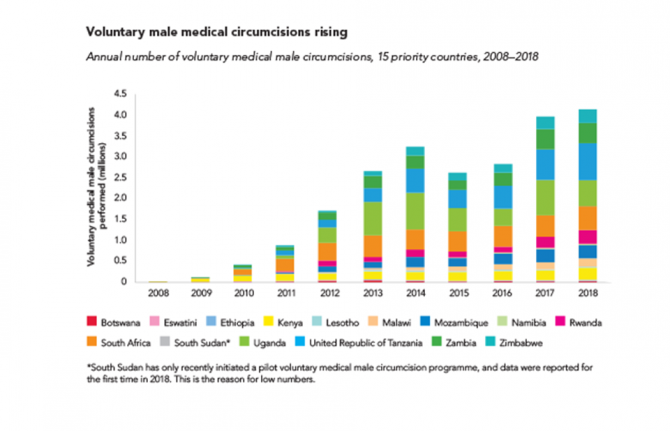
Voluntary medical male circumcision―4.1 million performed in 2018
21 October 2019
21 October 2019 21 October 2019Voluntary medical male circumcision (VMMC)―the removal of all or part of the foreskin of the penis by a trained health-care professional―reduces heterosexual male vulnerability to HIV infection by approximately 60%. Its effects last a lifetime. VMMC is also an entry point for providing men and boys with broader health packages to improve their health, and indirectly benefits women and girls.
VMMC can have a major impact on HIV epidemics in high-prevalence settings. VMMC services incorporate a package of prevention interventions, including safer sex education, education on and provision of condoms, HIV testing and the management of sexually transmitted infections.
About 11 million VMMCs have been performed in 15 priority countries in eastern and southern Africa since the beginning of 2016. In 2018 alone, about 4.1 million voluntary circumcisions were performed among males of all ages, a slight increase from the 4 million carried out in 2017.
There has been progress towards the target of 25 million additional circumcisions for HIV prevention from 2016 to 2020. However, at the end of 2018, when 15 million circumcisions should have been performed, the world was off-target by 4 million circumcisions.
Related
Government ensures continuity of treatment in Malawi
10 February 2025