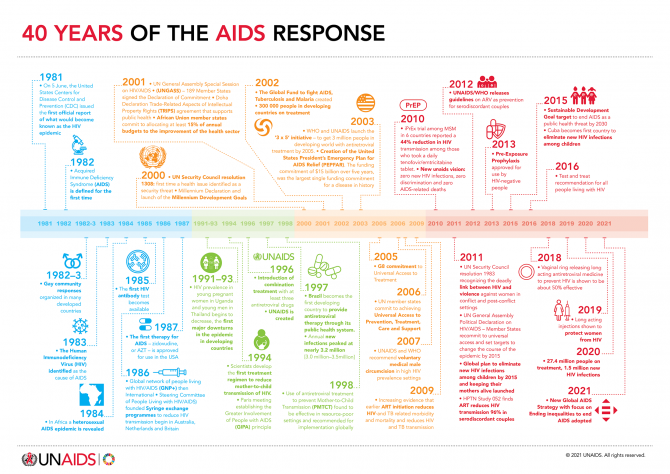
40 years of the AIDS response
Sex workers and clients

 and moderated by the Caribbean Community (CARICOM) Assistant Secretary-General, Douglas Slater")
, Diana Weekes noted that key structural barriers continue to block access to HIV prevention, treatment and care services.")



08 June 2021
08 June 2021 08 June 2021Caribbean partners from governments, civil society and the development community met on 7 June to discuss regional priorities for the 2021 United Nations High-Level Meeting on AIDS and its resulting political declaration. The virtual Caribbean Caucus was hosted by the Pan Caribbean Partnership against HIV/AIDS (PANCAP) and moderated by the Caribbean Community (CARICOM) Assistant Secretary-General, Douglas Slater.
The PANCAP Director, Rosmond Adams, noted that the Caribbean has made significant progress in key aspects of the HIV response. Eight countries and territories have been validated by the World Health Organization for eliminating vertical HIV and syphilis transmission. And between 2010 and 2020, AIDS-related deaths in the region fell by half (51%).
But to get on track to end AIDS by 2030, he said Caribbean countries must step up the pace around prevention, testing, treatment, care and ending stigma and discrimination. By 2020, 82% of people living with HIV in the region were diagnosed. Two thirds (67%) of all people living with HIV were on treatment and 59% were virally suppressed.
While new HIV infections have fallen by 28% since 2010, the rate of decline is too slow. Overall, members of key population communities and their partners accounted for 60% of new HIV infections in 2020. Around one third of new HIV infections were among young people aged 15–24 years.
Speaking on behalf of the Caribbean Regional Network of People Living with HIV (CRN+), Diana Weekes noted that key structural barriers continue to block access to HIV prevention, treatment and care services. These include “stigma and discrimination … lack of privacy, breach of confidentiality and limited redress” when people’s rights have been violated. She noted that no country in the region has adopted the CARICOM model antidiscrimination legislation, which was developed almost a decade ago. CRN+ called for greater emphasis on policy and legislative changes as well as community-led responses to address these structural barriers.
Ivan Cruickshank, the Executive Director of the Caribbean Vulnerable Communities Coalition, pointed to regional data that show that HIV disproportionately affects key populations, including gay men and other men who have sex with men, transgender people, sex workers and people who use drugs.
“According to the latest UNAIDS report, nations with progressive laws and policies, as well as robust and inclusive health systems, have had the best HIV outcomes. We must therefore create inclusive societies in which people are confident in their ability to seek medical treatment and exercise their social and economic rights. We must go beyond declarations, to remove laws that continue to criminalize communities and limit young people’s access to sexual and reproductive health and rights,” Mr Cruickshank said.
The Guyana Health Minister and Caribbean representative on the UNAIDS Programme Coordinating Board, Frank Anthony, reaffirmed the region’s commitment to the HIV response, saying that “governments in the region stand ready to do their part in ending AIDS by 2030.”
He pointed to longstanding challenges in the region, such as “removing the legal obstacles that foster discriminatory practices” and “prevention sustainability.” But he also emphasized the new threat posed by COVID-19, noting that “finite financial resources had to be reprogrammed to meet these urgent demands.” He called for increased vaccine equity and a review of plans to transition countries in the region away from international HIV funding.
“We must use the platform available to us at this United Nations high-level meeting to ensure that we highlight our vulnerabilities to the HIV epidemic and the COVID-19 pandemic,” he said.
During discussions, civil society participants also emphasized the profound negative impact of COVID-19 containment measures on lives and livelihoods. They said there was an additional need for solutions to provide nutrition, mental health and financial support to people living with HIV and members of key population communities.
The Director of the UNAIDS New York Liaison Office, César Núñez, noted that in the response to both HIV and COVID-19, the role of communities is clear.
“The response must include a key role for civil society at the table when frameworks are being put together and implemented,” he said.
Mr Núñez ended by calling for CARICOM’s support in securing an ambitious, action-oriented and laser-focused political declaration.

02 June 2021
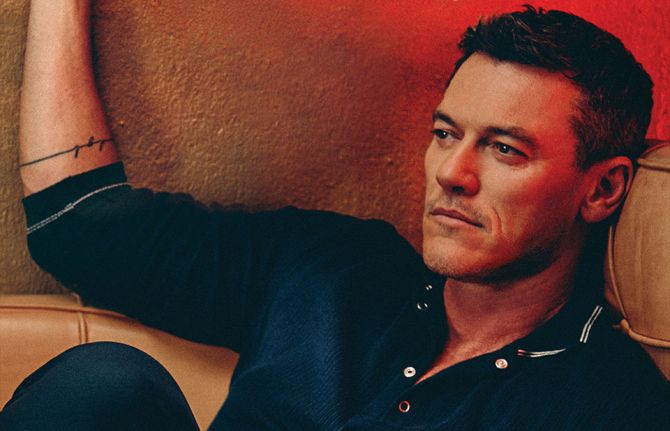
02 June 2021 02 June 2021Holding her baby in her arms, Melody (Melody, pictured above, preferred to use just her first name for this story) fled her home in Harare, Zimbabwe, one night after policemen stormed in and fatally shot her husband.
“I didn’t know my husband was a criminal. One night when we were sleeping, police barged into our home and killed him,” she says.
Terrified for her own life and without any money, she sought refuge with Emma Mambo, pictured below, a peer educator and community activist in Epworth, south-east of Zimbabwe’s capital.
Ms Mambo, affectionately known as MaiTino, volunteers with Katswe Sistahood, an organization that seeks to empower young women and girls in claiming their sexual and reproductive health and rights. She works extensively with women in her community, including sex workers. She also runs a dance and drama group for adolescent girls and young women, which explores the complex issues they face through the arts.
“I don’t get paid for my work, but I love Katswe because it elevated me and made me realize I can teach and work with people. Even when I get phone calls at night for help, I don’t mind,” she says. This is despite not being formally employed and raising her daughter, Tanaka, pictured below, as a single mother.
“Some of the circumstances these women face hurt me. I even use my own money to help them even though I am struggling myself,” she continues.
After fleeing her home, Melody struggled to make ends meet for herself and her child. Soon, she went back to sex work, a life she had left behind when she got married.
Sex work for Melody and other Zimbabwean women is a difficult and dangerous industry in which to work. While gender-based violence is a global epidemic, affecting one in three women worldwide, its impacts are exacerbated for sex workers.
Zimbabwe is one of the 103 countries worldwide in which sex work is criminalized, leaving sex workers unprotected by the law and exposed to a range of human rights violations.
Studies show that sex workers often face violence from the police, clients and partners, increasing their risk of acquiring HIV. Prevalence of HIV among sex workers in Zimbabwe is exceptionally high, estimated at 42.2%. Sex workers also face stigma and discrimination or lack of privacy from health-care workers.
Says Ms Mambo, “Going to the clinic is a procedure often void of actual medical care and dignity. This is particularly true if you are a sex worker with a sexually transmitted infection. Health-care workers will spread the news.”
This can also be true of HIV treatment. Ms Mambo helped a young sex worker go for HIV testing and counselling, only to find out that she had absconded when she was supposed to collect her treatment.
“When I eventually spoke to her, she told me that the clinic has no privacy. Everyone would be able to see her get her medication. I then helped her get a transfer to collect medication elsewhere,” she says.
Working as a sex worker in Harare, Trish (Trish, pictured below, preferred to use just her first name for this story) is familiar with the dangers of the trade, including gender-based violence. Clients often misuse alcohol and become violent towards sex workers.
“When I think back to last week, I couldn’t leave my home. My eye was so swollen. You get hit to the extent that you get injured. If you report it to the police, the client can bribe his way out without the matter being even heard. You are seen as lowly and powerless because you are a sex worker,” she says.
Police also harass sex workers from doing their job, said Ms Mambo, who often gets phone calls from sex workers in jail.
“Sometimes police go into a bar and demand that everyone lies on the floor, start searching people and start beating them. If you are unlucky, they can arrest you,” she says.
Living in the reality of arrests and assault, Melody said poverty is the only reason that drove her to be a sex worker, a line of work she entered at 19 years old. Following the death of her first husband, she momentarily escaped the trade when she fell in love with a man with a formal job who could afford to look after her and her child.
However, that was short lived as her second partner was arrested for stealing from his workplace.
“I have nothing against my last partner who got arrested,” Melody says. But she has still not been able to shake off the tainted reputation she got from her first husband.
“When I am working in bars, police come and harass me because of who my first husband was,” Melody says. “The police should leave us to work freely outside of abuse. Our children need to eat and our parents need to be taken care of,” she insists.
Her personal and work experiences with men have negatively affected Melody’s perception of men. However, she says she does not fully express her pain because these are the very men who can provide her next meal.
She does not want it to be like this forever, though. “I’d be happy to get a better job that won’t expose me to danger,” she says.
Ms Mambo also dreams of a life beyond her current circumstances. “Someone offered me a piece of arable land to farm on. I am looking for fertilizers to farm potatoes because sex work and my age don’t correlate anymore,” she says.

24 February 2025
20 February 2025

26 April 2021
26 April 2021 26 April 2021Viral hepatitis infection is a major global public health problem causing approximately 1.4 million deaths per year—more than the annual number of AIDS-related deaths. Ninety-six per cent of these deaths are from cirrhosis and hepatocellular carcinoma due to hepatitis B and C viruses, which are transmitted via blood and body fluids.
People living with HIV and hepatitis B or hepatitis C coinfection have a more rapid progression to cirrhosis. Liver disease has emerged as an important cause of death among people living with HIV coinfected with either hepatitis B or hepatitis C.
Hepatitis C coinfection with HIV is reported across all key populations at higher risk of HIV, especially among people who inject drugs. This is due to the ease with which both viruses are spread through the sharing of non-sterile drug preparation and injecting equipment.

24 March 2021
24 March 2021 24 March 2021After years, their wait is over. The Association des Femmes Amazones Zen (AFAZ) has opened a drop-in centre in Lomé, the capital of Togo, where female sex workers can find refuge and help.
Funded by the United States President’s Emergency Plan for AIDS Relief through the Ending AIDS in West Africa project implemented by FHI 360, the centre opened last October, providing HIV prevention and testing services, the treatment of sexually transmitted infections, care for people living with HIV and assistance to survivors of gender-based violence.
Honorine Têlé Mensah, the coordinator of AFAZ, said that such drop-in centres bring many benefits for the community. The centre provides people with a place where they can listen, receive information and training and meet and share with others. It is a place where they can feel safe and free from discrimination and stigma. “By helping women to speak out and feel confident, we help them set an example for the community. In this way, the centre has an impact on the entire community,” she said.
But she has encountered difficulties. “Some people don’t want to get tested, and we sometimes lack nutritional kits to assist people living with HIV to stay on treatment and items such as reagents for HIV testing. Restrictions due to the COVID-19 pandemic have not helped either.” According to her, funding should be reviewed and the provision of items such as nutritional kits should be taken into account.
“I would like all AFAZ members in Togo to be able to benefit from drop-in centres and care centres like in Lomé,” she said. In the future, she would like the centre to grow. “It would be great if members could benefit from training in entrepreneurship or income-generating activities,” she said.
“Drop-in centers are often the only places where sex workers can access health care, legal advice and other services. They also provide a safe space for sex workers to gather, document abuses and mobilize for their rights,” said Eric Verschueren, UNAIDS Country Director for Togo. “UNAIDS supports the opening of more across the country.”
19 February 2025



24 March 2021
24 March 2021 24 March 2021Located in Bole sub-city, the Bole drop-in centre is one of 12 such centres established in Addis Ababa, Ethiopia, to provide community-based comprehensive HIV services. It provides critical services and support for clients, including female sex workers, and has been a lifeline during the COVID-19 outbreak.
The centre offers a full range of integrated clinical services, including HIV testing and self-testing kits, the provision of oral pre-exposure prophylaxis (PrEP), antiretroviral therapy, the diagnosis and treatment of sexually transmitted infections, screening and referral for the treatment of tuberculosis, cervical cancer screening and treatment, and programmes to prevent and respond to gender-based violence, including access to post-exposure prophylaxis.
The drop-in centre is strategically located in one of the city’s hotspots to cater primarily for female sex workers and their children, young women and adolescent girls who are out of school, and men at higher risk of HIV infection.
It also offers consultations by mobile phone, with 31 cyber-educators trained to provide 15-minute counselling sessions with an accent on the prevention of both HIV and COVID-19. The programme has proved to be invaluable during the COVID-19 pandemic.
“I am truly inspired by the work being carried out at the Bole drop-in centre,” said UNAIDS Executive Director, Winnie Byanyima, when she met staff and clients during her recent visit to Ethiopia. “It is a great example of integrated community-led service delivery and is exactly the kind of programme that is key to ending AIDS as a public health threat by 2030.”
The centre is primarily funded by the United States President’s Emergency Plan for AIDS Relief, through the United States Agency for International Development, while UNAIDS has provided catalytic funding for the cyber-education programme, the promotion of PrEP among vulnerable groups of people and mental health counselling. This support will help to generate the uptake and continuation of needed services during the COVID-19 pandemic. Partners include Population Services International and a local nongovernmental organization called Integrated Service on Health and Development Organization.
As the measures taken to contain COVID-19 continue to bite, the Bole sub-city drop-in centre will remain a critical service for female sex workers and their families.
“During the COVID-19 lockdown, many sex workers found it difficult to work and the drop-in centre has been their only source of food,” said Sister Desta Franso, an antiretroviral provider and counsellor at the clinic.
Up to 20 female sex workers use the centre every day and around 140 women are receiving HIV medication. Treatment retention at around 94% is extremely high.
“I am so happy to be able to come here to get free medication and condoms,” says Mekdes Matiyos, a regular user of the clinic. “I can also just come to take a shower and rest whenever I need to, and I don’t have to pay.”
24 February 2025
20 February 2025

12 January 2021
12 January 2021 12 January 2021Warm smiles greet Lily as she approaches her first stop of the day—one of the 11 brothels scattered across the country that Lily, the President of the Bangladesh Sex Worker Network, visits quarterly to check in with the women and see what assistance they need. Though her visits have been limited in recent months due to movement restrictions to curb the spread of COVID-19, Lily knows well enough that those smiles are a brave front for the troubling times that her peers have experienced.
“I see the sex workers as my sisters—I feel their happiness and pain and I try my best to solve any issue they face,” Lily said. During the COVID-19 pandemic, Lily and the 29 community-based organizations serving sex workers in the country have struggled to respond to the increased calls for support. In March, government countrywide movement restrictions meant that sex workers could no longer have clients, leaving most of them without a source of income and unable to provide for themselves or their families.
“Sex workers’ children faced challenges during the COVID situation because their mothers couldn’t arrange to provide them with food. When we [the Bangladesh Sex Worker Network] learned about this issue, we reached out to many organizations and the private sector for assistance,” explained Lily. Responding to the call to action, the network mobilized funds to support 2100 sex workers across the country. Community-led support in Bangladesh has also garnered global recognition. Most recently, a former sex worker, Rina Akter, was recognized by the BBC for her efforts, and those of her team of helpers, to serve 400 meals a week to sex workers in need.
“While a few sex workers had savings, most could not provide for themselves,” said Rahat Ara Nur, Technical Officer for the United Nations Population Fund in Bangladesh. “Through the United Nations Population Fund, we provided sex workers with COVID-19 prevention commodities, such as masks and handwashing materials, and we also developed public service announcements which were aired on community radio to ensure we raised awareness about COVID-19 precautionary measures among the community."
With the closure of entertainment venues, a classification that includes brothels, some sex workers have resorted to street-based sex work, which increases the risk of violence, condom-less sex and no pay or low pay.
Sex workers are also experiencing increasing vulnerability to gender-based violence. Without a source of income, conflicts about finances arise, and sex worker networks report that their members have experienced abuse at the hands of their spouses, partners and brothel owners.
Some sex workers report that they have become homeless because the brothels have been closed, or in some cases the residents were evicted because rent could not be paid. Many sex workers cite stigma and discrimination as a barrier for other forms of employment. Health outreach services that once provided brothels with sexual and reproductive health services, including HIV testing and prevention, have been suspended due to travel restrictions.
Bangladesh, October 2019. Credit: UNFPA Bangladesh/Naymuzzaman Prince
These developments are not unique to Bangladesh, however. Throughout the Asia–Pacific region, national and regional networks of sex workers are reporting that the COVID-19 outbreak has exacerbated the inequalities faced by sex workers, and many are either not eligible or excluded from social protection services.
“There is no government support specifically targeting sex workers. There is support for the general public, particularly those that are low income, but sex workers are not eligible for these social protections because they work in the informal economy,” said Hnin Hnin Yu, the Chairperson of Sex Workers in Myanmar (SWiM), a nongovernmental advocacy group for sex workers’ rights.
Additionally, many sex workers are migrants (international or internal) and lack the necessary papers or registration with local authorities to access the government’s support. Eligibility criteria for social support, such as documentation of income, proof of residence, national identification, contribution to existing social protection schemes and filing taxes, are all reasons given for excluding sex workers from government support. An online consultation of female sex workers from across the country, organized by UNAIDS and SWiM, revealed that apart from limited funds from humanitarian actors, none of the sex workers had received social support.
“When Global Fund to Fight AIDS, Tuberculosis and Malaria assistance for COVID-19 was allocated, funds for people living with HIV included the most vulnerable sex workers to receive food provisions,” said Mr Myo, Community Support Adviser for UNAIDS in Myanmar. “However, we recognized that this was an ad hoc solution that reached a small portion of the vulnerable population and there is a need for more sustainable support, such as social protection, for sex workers.”
It has become clear that focused support for sex workers must be prioritized. Recognizing that more needs to be known about the gaps in social protection for sex workers, UNAIDS in collaboration with the United Nations Population Fund and the World Food Programme are exploring the possibility of conducting a needs assessment and vulnerability mapping initiative of female sex workers during the COVID-19 pandemic. Data from the community-led mapping initiative will be used to inform programming for livelihood support, food security, improved access to antiretroviral therapy, sexual and reproductive health services and gender-based violence prevention and response services.
Commenting on the prospects of the United Nations agencies joining forces to coordinate a vulnerability mapping exercise with sex worker networks, Ms Nur expressed excitement about how this advocacy tool will not only help to identify the challenges that sex workers face during the COVID-19 outbreak, but it would also catalyse further work to mobilize resources for programmes and address injustices that pre-date the COVID-19 pandemic.
Hnin Hnin Yu cites discrimination and harassment from police as a long-standing challenge facing sex workers’ rights. During the COVID-19 outbreak, communities have reported increased police surveillance, harassment, including physical violence, and demands to pay fees to conduct sex work. In response, SWiM provides community-led, peer-to-peer legal aid for sex workers who have been arrested, educating them about their rights.
For those working closely with community-led organizations it has been inspiring to see that although sex worker networks and the sex workers they represent have seen challenges all around them, they have done their best to support their peers. There is hope that the data gathered in a vulnerability mapping exercise would not only generate the evidence needed to advocate for expanding the reach of social protection and humanitarian response services to be inclusive of sex workers, but could also inform the scale-up of community-led programming.
24 February 2025
14 January 2021
This report provides a summary of key developments in the legal environment for HIV responses in Asia and the Pacific. It is the product of a desk review conducted for UNAIDS and the United Nations Development Programme (UNDP) in 2019. The report highlights key trends and developments in laws affecting people living with HIV and key populations in Asia and the Pacific over the five-year period 2014–2019. It updates the legal and policy review conducted in 2016 for UNAIDS, UNDP and the United Nations Economic and Social Commission for Asia and the Pacific (ESCAP). A database of laws of the 38 Member States of ESCAP was created as part of this review. The database identifies laws that are either punitive or enabling for people living with HIV and key populations in Asia and the Pacific. A summary of the findings is presented in Annex 1. An overview poster is also available.

24 February 2025
30 January 2025

21 January 2025
21 January 2025
17 December 2024
02 December 2024

GENEVA, 10 December 2020—UNAIDS announces the launch of its Solidarity Fund, which will support social entrepreneurs and micro-business owned by key populations facing special hardship during the COVID-19 pandemic.
“Key populations are among those disproportionally impacted by COVID-19,” said Winnie Byanyima, UNAIDS Executive Director. “COVID-19 has highlighted and exacerbated the profound and widening economic and social inequalities. We must act to support and protect the people who are most impacted by the pandemic.”
Experience from the COVID-19 and HIV pandemics, and from other diseases, such as Ebola, has shown that key populations are more likely to be impacted by food insecurity, face barriers to health care and access to medicines, and suffer losses of livelihood, unemployment, homelessness and domestic violence.
Launched today, Human Rights Day, the new Solidarity Fund will support social entrepreneurs and small-scale businesses owned by people living with HIV, women or members of key populations, including sex workers, transgender people, people who use drugs and gay men and other men who have sex with men, the people who so often have their human rights violated.
“The fund will help bridge the gap between aspirations and opportunities of people from my community. It places trust and gives us a chance to show our innovation and entrepreneurship with no limitations,” said Maite Schneider, the cofounder and Chief Executive Officer of TransEmpregos.
To be piloted initially in five countries—Brazil, Ghana, India, Madagascar and Uganda—with a US$ 250 000 budget from UNAIDS, the initiative will scale up to additional countries over the coming months, with a goal of raising an additional US$ 3 million to US$ 5 million in 2021–2022.
UNAIDS will closely work with community networks, national innovation ecosystems, the private sector and other partners to create tailored support, especially capacity development on social entrepreneurship and mentoring to enhance the sustainability of social ventures and impact for the wider community, with special attention given to young key populations.
Among the partners is the venture development and investment platform Social Alpha, which will provide mentoring and entrepreneur support to the chosen beneficiaries. “We look forward to partner with communities and UNAIDS on the Solidarity Fund and leverage our experience in working with social entrepreneurs for solving complex social, economic and environmental challenges,” said Manoj Kumar, the Chief Executive Officer and founder of Social Alpha.
UNAIDS
The Joint United Nations Programme on HIV/AIDS (UNAIDS) leads and inspires the world to achieve its shared vision of zero new HIV infections, zero discrimination and zero AIDS-related deaths. UNAIDS unites the efforts of 11 UN organizations—UNHCR, UNICEF, WFP, UNDP, UNFPA, UNODC, UN Women, ILO, UNESCO, WHO and the World Bank—and works closely with global and national partners towards ending the AIDS epidemic by 2030 as part of the Sustainable Development Goals. Learn more at unaids.org and connect with us on Facebook, Twitter, Instagram and YouTube.
Download the printable version (PDF)

26 October 2020
26 October 2020 26 October 2020There are significant gaps in HIV testing among key populations at higher risk of HIV infection, resulting in suboptimal levels of knowledge of their HIV status. HIV testing is a critical gateway to HIV prevention and treatment services. Without knowledge of HIV status, people cannot access life-prolonging HIV treatment services.
Analysis of data from special surveys shows that, on average, about two thirds of sex workers and gay men and other men who have sex with men globally either had taken an HIV test and received the results within the past 12 months or had previously tested positive for HIV—meaning that about one third did not know their HIV status. This testing gap was even larger for people who inject drugs. These surveys are often conducted where key population-friendly services are available and may overstate overall testing coverage.