

Feature Story
A bond of intimacy, free from HIV
06 June 2019
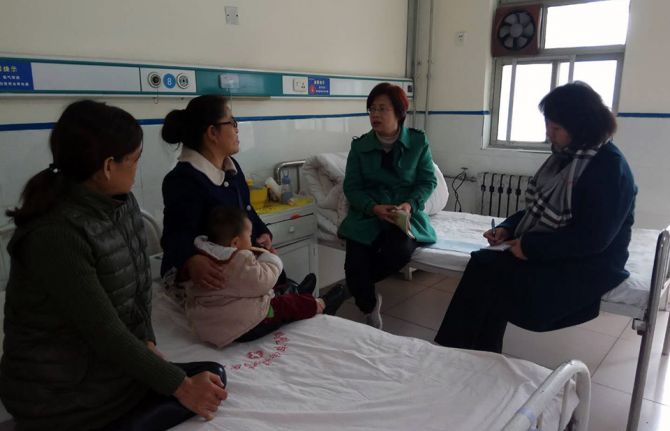
06 June 2019 06 June 2019“I thought I could never be happy again,” said Mei Zi, who is living with HIV and a mother of a lively young boy. She calls her son “calm angel”, as he doesn’t talk much. Mei Zi says that “calm angel” as a gift from God.
Mei Zi met her husband two years after she discovered that she was living with HIV. After their wedding, she went to live with her husband in Beijing, China, where he worked. She remembers receiving a red down jacket as a present from her husband when she got off the train in Beijing. The excitement is still fresh, even though it was a long time ago.
Soon after her marriage, Mei Zi became pregnant. Although her doctor advised her that she could take medicine to ensure that her baby was born free from HIV, she made the painful decision to terminate the pregnancy. She and her husband were both living with HIV and, in addition, she was living with hepatitis C.
Mei Zi put having children out of her mind, but five years later a test showed that she was pregnant.
Mei Zi was treated just like any other expectant mother at the hospital. She decided to take treatment to stop her baby becoming infected with HIV and to treat her hepatitis after the baby’s arrival.
Because of the hepatitis, Mei Zi had a cesarean section in the 34th week of her pregnancy. She was afraid of the surgery, but eager to see her baby.
“As the door of the operating room was pushed open, I started crying,” said Mei Zi. “I felt the door was just like between life and death.” When the doctor presented her with the new arrival, she could not believe it was true―a healthy baby boy, free from HIV.
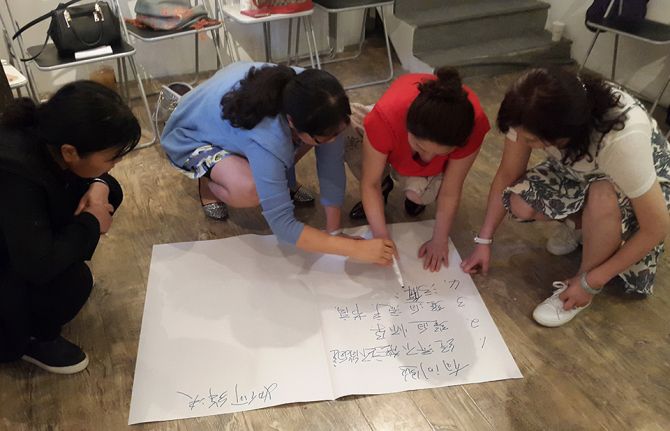
The Women’s Network against AIDS in China (WNAC) is striving to ensure that more women living with HIV and hepatitis C are aware that they can have healthy children and receive the support to do so.
WNAC was established in 2009 with assistance from UNAIDS and consists of 27 women’s community organizations across 12 provinces in China. It is a platform that brings together and advocates for women living with HIV and ensures that women living with HIV get the help and support they need to access appropriate health care and give birth to babies free from the virus.
Mei Zi achieved her dream of having a healthy baby, but it was not by chance. The support she received from her health-care provider, WNAC, organizations in the network and many other community groups made it possible.
“Calm angel” is now four and a half years old and energetic and curious about the world.
Region/country




Feature Story
Malawi: remember where we have come from to move forward
05 June 2019
05 June 2019 05 June 2019Dan Namarika, the Principal Secretary for Health in Malawi, graduated from the College of Medicine in 1999 as one of the first students to follow their entire medical training in Malawi. His long career as a medical doctor, which included four years as personal physician to the late President Bingu wa Mutharika, was prompted by a desire to act against AIDS.
“The reason I chose medicine was because of AIDS. I couldn’t believe there was an illness like this with no cure. I remember the first case in my neighbourhood. It was a lady who succumbed to AIDS after a chronic illness. I have had family members that have died. My long history has been impacted on by AIDS,” he says.
Since the peak of the HIV epidemic to which Mr Namarike refers, when there were 110 000 new infections (in 1993 and 1994) and 65 000 deaths because of AIDS-related illnesses (in 2004 and 2005), Malawi has made good progress in its HIV response.
This progress can be attributed to the introduction of innovations such as the test and start strategy in 2016, which offers immediate HIV treatment for all people living with HIV and Option B+ in 2011, a prevention of mother-to-child transmission of HIV strategy that ensures that all pregnant women living with HIV have lifelong access to HIV treatment.
As a result, new HIV infections in Malawi have dropped by 40%, from 64 000 in 2010 to 39 000 in 2017, and AIDS-related deaths by half, from 34 000 in 2010 to 17 000 in 2017. Life expectancy continues to rise, from a mere 46 years in 2004 to 64 in 2018, and projections are that it will rise to 74 by 2030.
In 2017, 92% of pregnant women living with HIV in Malawi accessed services to prevent mother-to-child transmission of HIV. This lowered the number of new HIV infections among children (0–14 years) to an all-time low of 4900 in 2017.
Mr Namarika attributes these successes in large part to the multisectoral HIV response and high-level political commitment and leadership. “Besides policies being made at the highest levels of government, we also have ministries other than health involved, such as the treasury, gender, education and local government; we have civil society, the faith-based sector, cultural leaders and technical assistance from development partners, such as UNAIDS,” he says.
He also praises programmatic innovations, such as task shifting from doctors to nurses and community health-care workers, which has helped to reach more people with HIV testing and treatment services.
The 2015–2020 National Strategic Plan for HIV and AIDS has the 90–90–90 targets at its heart, with ending AIDS by 2030 in Malawi as the end goal. Malawi has made good progress in the number of people living with HIV who know their status (90%) and the number of people living with HIV who are on HIV treatment (71%). More work is needed to increase the number of people living with HIV who have suppressed viral loads (61%), which puts Malawi at risk of not meeting the targets in the next 500 days.
The major obstacle to Malawi’s progress in meeting the targets, according to Mr Namarika, is people being left behind because of socioeconomic and structural disparities driven by power relationships, such as poverty, unemployment and gender inequality. He also believes that a location–population approach is needed to address vulnerabilities exacerbated by migration and natural disasters, such as the drought–flood cycle experienced by people located in the south-east of the country.
Another challenge in the national AIDS response is high new HIV infections among adolescent girls and young women between the ages of 15 and 24 years, who accounted for 9500 new infections in 2017—more than double that of their male counterparts (4000).
“Most young people cannot make ends meet. This puts girls most at risk—their rights can be easily trampled on by older men. Also, health-seeking behaviour among young men needs to be improved,” says Mr Namarika.
However, Mr Namarika believes that the biggest obstacle to progress in the AIDS response is complacency.
“When I was a young medical doctor on some days we would have 19 deaths just in the paediatric ward alone. Not in the whole hospital, just in that one ward. Now, the young doctors don’t see that anymore, so they don’t believe that HIV is real,” he says.
He believes that it is critical to continue to engage with communities on AIDS with the same urgency that there was in the early 2000s, so that the significant gains that the country has made are not lost.
“If the cost of AIDS is not regarded as one of the biggest historical disasters we have experienced in the 54 years of our independence, then we have lost our history,” he insists.
The way forward primarily is to continue financing the AIDS response and to put more emphasis on HIV prevention. This will require a growing domestic investment, as well as convincing development partners to put more external sources of funding into HIV prevention, he says.
Related information
Region/country









Feature Story
Young women demand accountability at Women Deliver
05 June 2019
05 June 2019 05 June 2019It has been 25 years since the groundbreaking International Conference on Population and Development, held in Cairo, Egypt, in 1994. Since then, significant progress has been made in the area of sexual and reproductive health and the rights of young women and adolescent girls. Voluntary access to modern contraception has increased by 25% since 1994, and the quality of sexual health and HIV services has also vastly improved.
So why are around 7000 young women and girls still becoming infected with HIV every week? And why, in sub-Saharan Africa, are girls aged 15–19 years three times as likely to become infected with HIV than boys the same age?
“We cannot wait another 25 years. We need to push for accountability to make sufficient progress in addressing the current government deficit to deliver on the sexual and reproductive health and rights commitments for women and girls,” said Gogontlejang Phaladi, from the Pillar of Hope Project in Botswana.
Her comments set the tone at an event organized by the Global HIV Prevention Coalition, during the Women Deliver conference in Vancouver, Canada. The event, co-convened by UNAIDS and the United Nations Population Fund (UNFPA) and held on 3 June, put the spotlight on why young women and adolescent girls are being left behind and why they continue to bear the brunt of poor sexual and reproductive health and HIV.
“We are facing an HIV prevention crisis,” said Shannon Hader, UNAIDS Deputy Executive Director, Programme. “While the target was to reduce new HIV infections among adolescent girls and young women to fewer than 100 000, an estimated 340 000 became newly infected with HIV in 2017. We have a huge task ahead of us.”
Speakers at the event discussed the critical importance of engaging young people as leaders of change. “We need to call out policy-makers, traditional and religious leaders, even parents,” said Monica Geingos, First Lady of Namibia. “We must never tell you what to say. Generations before, you were shamed and silenced. Never lower your voices.” She also added that the lack of progress for women and girls is being fuelled by gender discrimination, violence and denial of fundamental freedoms.
UNFPA’s Regional Director for Eastern and Southern Africa, Julitta Onabanjo, also stressed that more needs to be done. “I see a dynamic young women warrior generation here to take the agenda forward—so that by 2030 every young person can fulfil their best potential and nothing is going to hold them back,” she said, while noting that the recommendations of the event should be fed into a summit being held in Nairobi, Kenya, later in 2019.
A major issue preventing young women and girls from accessing HIV services is the requirement by many countries that young people have to be over the age of 18 before they can access health services, including sexual and reproductive health and HIV services, without parental consent. UNAIDS estimates that 78 countries have some form of restrictive laws or policies that prevent young people from accessing sexual health services without the consent of their parents.
As part of efforts to remove these barriers to young people accessing timely and effective HIV prevention, testing and care, during the youth-led Generation Now: Our Health, Our Rights preconference meeting on 2 June, UNAIDS committed to tackle parental consent laws, and their implementation, in five countries in eastern and southern Africa—Lesotho, Malawi, Namibia, Uganda and Zambia. This includes working with young people to ensure that youth are driving change and co-creating the quality services they want and need to have bright and healthy futures.
To advance progress, the participants agreed that investing in community organizations will be critical, as will taking small projects that work to the national level. Nyasha Sithole, from the Athena Network said, “People are watering the leaves, but not the roots. We need to move away from paper and pen to implementation on the ground.”
UNAIDS is a co-convener of the Global HIV Prevention Coalition, which works with countries with a high incidence of HIV to accelerate access to combination HIV prevention services. The coalition seeks to ensure accountability for delivering HIV prevention services at scale in order to achieve the targets of the 2016 United Nations Political Declaration on Ending AIDS, including a 75% reduction in HIV infections towards fewer than 500 000 new infections by 2020. The work of the coalition includes a particular focus on young women and their male partners.





Feature Story
Chisinau signs the Paris Declaration
04 June 2019
04 June 2019 04 June 2019Ruslan Codrenu, the Acting Mayor of Chisinau, Republic of Moldova, signed the Paris Declaration to end the AIDS epidemic in cities on 31 May. He committed the city to achieving the 90–90–90 targets by 2020, whereby 90% of all people living with HIV know their HIV status, 90% of people who know their HIV-positive status are on treatment and 90% of people on treatment have suppressed viral loads. The city will specifically focus on marginalized and vulnerable people and on ending stigma and discrimination.
“Achieving 90–90–90 will be difficult, but it is never too late to start making the necessary changes to improve people’s lives and health. Today, the city authorities commit to significantly increasing the coverage of the residents of Chisinau with HIV prevention, testing and treatment services, with the aim of ending the AIDS epidemic and concentrating efforts on programmes for key populations,” said Mr Codrenu.
Mr Codrenu said he expects that a new municipal HIV control programme for 2019–2020 will soon be adopted by the city council. The programme will focus on additional HIV testing and treatment for approximately 750 people living with HIV and the provision of HIV prevention services for key populations.
“Chisinau must move quickly, not only to reach 90–90–90, but also to eliminate discrimination against people living with HIV and key populations, which remains a significant barrier. In this struggle, our city is not alone. Chisinau is supported by a team of regional and national leaders who are willing to share their expertise,” said Svetlana Plamadeala, UNAIDS Country Manager for the Republic of Moldova.
Chisinau already supports a range of HIV prevention programmes for key populations, including harm reduction and opioid substitution therapy programmes for people who inject drugs, rapid HIV testing and condom distribution for sex workers and their clients and condom distribution among gay men and other men who have sex with men. However, it is planned that with the adoption of the new municipal HIV control programme, the quality, coverage and impact of the programmes will be significantly enhanced.
Chisinau is the seventh city in eastern Europe and central Asia to sign the Paris Declaration, which since 2014 has been signed by more than 300 cities worldwide.
The signing of the Paris Declaration in Chisinau is the most recent result of a long history of effective cooperation between national, state and nongovernmental organizations, regional networks representing key populations and international organizations
According to government estimates, there are about 3200 people living with HIV in Chisinau.
“Today, we witness what can be achieved through political will. It is of paramount importance to us that the Paris Declaration is not another declarative statement, but is followed by the adoption of the municipal HIV programme, with specific and measurable goals and roles and a budget,” said Ruslan Poverga, General Director of the Positive Initiative.
Related information
Region/country
Related




Feature Story
Changing the lives of transgender people in Malawi
03 June 2019
03 June 2019 03 June 2019Lesbian, Intersex, Transgender and other Extensions (LITE) started out in 2016 as a support group for lesbian, gay, bisexual, transgender and intersex (LGBTI) people in Lilongwe, Malawi. “There was so much commonality in the challenges facing lesbian, gay, bisexual, transgender and intersex people that this motivated me to form a nongovernmental organization addressing these issues,” says Lawrence Phiri Chipili, Executive Director of LITE, who is a transgender man.
Since its formation in 2016 and its formal registration in 2017, LITE has navigated its way into important national platforms, including the Malawi National AIDS Commission’s technical working group that guides the multisectoral AIDS response.
In May 2019, LITE, along with five other LGBTI organizations in Malawi, formed the Diversity Forum to collaborate on their common goal of ensuring that LGBTI rights are promoted, protected and respected in Malawi. LITE is also the Deputy Chair of the Southern Africa Trans Forum, which brings together 18 transgender organizations from the Southern African Development Community. In 2019, LITE and Mr Chipili were recognized by the Human Rights Campaign as one of their global innovators.
None of this recognition has come easy to the organization. Using his academic background in economics, Mr Chipili has pushed for evidence to support the organization’s advocacy.
“We decided as we were forming the organization that we needed a baseline understanding of what the needs of transgender people are in both the rural and urban areas of Malawi,” he says. “We didn’t want to base our assumptions on a small group of people living in Lilongwe. We conducted a needs assessment with communities and we realized the overarching challenges they have in accessing health-care services, education, employment, legal services and the enjoyment of safety and security.”
The research has helped the organization to design its advocacy strategy, which involves rendering transgender people’s issues visible in the public and policy space.
The organization also uses policy and the law to shape its advocacy. In 2015, the Malawian Government accepted that LGBTI people should have access to health and security. However, according to Mr Chipili, these recommendations are not implemented on the ground. Thus, using these recommendations as a basis, LITE designs its strategy to generate research so that it can strategically engage with the government.
No one knows more about these challenges better than Mr Chipili. He has been thrown out of home, school and university. His resilience and determination seem only to have grown stronger from his experiences.
“I risk my life; I risk the lives of people in my immediate circles, but these are problems that we experience in our everyday lives so we must speak about them. Hate speech towards my community pains my soul but it motivates me because people don’t understand the impact of their words. My mission is to work hand in hand with these people and help them to understand,” he says.
Mr Chipili acknowledges that while it has been a lone struggle by the LGBTI community to become more visible, the role of partners, including UNAIDS, has been critical. “UNAIDS has assisted us in understanding where our gaps are in our organizational policies and helping us to shape the direction in which we should go,” he says. “It has advocated for our inclusion in national platforms and helped us to strategically engage with the government, with the ethos of leaving no one behind firmly at the centre.”
The work has just started for Mr Chipili and his organization. “We need more technical support, human resources and financial resources. One of the major issues is transgender programming and funding globally is limited. A lot of resources are given to organizations that work with men who have sex with men and female sex workers,” he says. “Transgender people are usually invisible, yet we are the people who are experiencing so much hate and stigma, making us even more at risk of HIV infection,” he says.
Related information
Region/country
Related

 “Who will protect our young people?”
“Who will protect our young people?”
02 June 2025
 Impact of US funding cuts on HIV programmes in Malawi
Impact of US funding cuts on HIV programmes in Malawi
15 April 2025

Feature Story
The little-known links between cervical cancer and HIV
31 May 2019
31 May 2019 31 May 2019Cervical cancer is the most common cancer among women living with HIV. The likelihood that a woman living with HIV will develop invasive cervical cancer is up to five times higher than for a woman who is not living with HIV. The overall risk of HIV acquisition among women is doubled when they have had a human papillomavirus (HPV) infection.
So, what can be done? This is one of the questions that will be discussed at a number of events addressing cervical cancer at the 2019 Women Deliver conference, which will take place in Vancouver, Canada, from 3 to 6 June.
Like HIV, cervical cancer is a disease of gender and other inequalities. These two interconnected diseases starkly expose the links between inequity and social and health injustice. Ninety per cent of 311 000 cervical cancer deaths globally per year occur in low- and middle-income countries, with the highest burden borne by sub-Sahara African countries that have the highest burden of HIV. In Zambia, rates of cervical cancer are almost 10 times higher than in Australia, for example, and women are 10 times more likely to die of cervical cancer in eastern and southern Africa than they are in western Europe.
Cervical cancer is preventable and curable if diagnosed and treated early. Effective methods of primary prevention of cervical cancer, notably the HPV vaccine, are available, but not to everyone. Currently, just 10% of girls in low- and middle-income countries access the HPV vaccine, compared with 90% in high-income countries.
Scale-up is happening and efforts to prevent and treat cervical cancer are showing dramatic results in areas where programmes have been rolled out at sufficient scale. Australia is set to become the first country in the world to eliminate cervical cancer by successfully implementing a combined approach to HPV vaccination and cervical cancer screening and early treatment at a wide scale. In Scotland in the United Kingdom, where the immunization programme was introduced some 10 years ago, there has been a 90% decrease in precancerous cells, which has led to a dramatic reduction in preinvasive cervical disease. Remarkable achievements, which should be universal.
“To save a woman’s life by ensuring that she has access to antiretroviral therapy for HIV, yet she dies from cervical cancer, is unacceptable,” said Shannon Hader, UNAIDS Deputy Executive Director, Programme. “UNAIDS’ focus is on breaking down silos and building bridges between HIV and cervical cancer programmes because we know that synergies save lives.”
Despite their increased risk of cervical cancer, women living with HIV do not receive regular screening or treatment for cervical cancer, even with the World Health Organization (WHO) recommended simple, low-cost visual inspection or effective simple, early treatment methods.
According to recent large studies, only 19% and 27% of women living with HIV aged 30–49 years in Malawi and Zambia, respectively, have ever been screened for cervical cancer.
A smart investment is to integrate cervical cancer screening and treatment services into HIV and sexual and reproductive health services. HIV platforms are ready-made entry points for low-cost cervical cancer services and wider health service coverage for young women and girls.
An important lesson learned from the AIDS response is that civil society and communities have to be at the centre. Networks of women living with HIV and women’s rights and youth movements are formidable allies. They have fought for an AIDS response rooted in human rights, social justice and sexual and reproductive health and rights and can mobilize, advocate and create demand for services. Civil society must also keep us on track to end stigma and discrimination, including in health-care settings. Communities can also provide direct services for HIV, cervical cancer and other diseases.
Shared responsibility and country leadership and ownership are critical. With collective efforts of governments, communities, donors, the private sector, innovators and researchers, important synergies can be made, and lives saved.
UNAIDS is working with partners to ensure that policies are informed by evidence, that ambitious targets are set and that adequate levels of human and financial resources are available. UNAIDS is using the political and programmatic platforms of the Fast-Track approach as part of the initiative to scale up the prevention and treatment of cervical cancer and HIV.
UNAIDS is working in partnership with initiatives such as WHO’s global call to action towards the elimination of cervical cancer and is part of a renewed Partnership to End AIDS and Cervical Cancer with the United States President’s Emergency Plan for AIDS Relief and the George W. Bush Institute.
“It is high time to make both AIDS and cervical cancer history!” added Dr Hader.
2019 Women Deliver conference
Related



 people in India.")


Feature Story
The road to equality for LGBTI people in India
24 May 2019
24 May 2019 24 May 2019“The job has just begun. We have come a long way, but we still have a lot to do.” That was the message from Ajit Prakash Shah, who delivered the Delhi High Court judgement in 2009 that led the way to the eventual annulling in 2018 of Section 377 of the Indian Penal Code, which criminalized same-sex sexual relations.
The retired Chief Justice of Delhi High Court was speaking at a meeting hosted by UNAIDS and partners in New Delhi, India, on 15 and 16 May on the rights of lesbian, gay, bisexual, transgender and intersex (LGBTI) people in India.
“Our aim is to mobilize and organize the community so they can together help each other,” said Bilali Camara, UNAIDS Country Director for India.
The speakers noted that despite recent legal judgements―including the annulling of Section 377 and the decision by the Supreme Court of India in 2014 on the rights of transgender people―the situation for LGBTI people in India had not changed drastically. However, it was noted that there is a perception that there is an increasing understanding of the issues of transgender people among the general public.
“The reason for the spike in crimes against lesbian, gay, bisexual, transgender and intersex people is partly due to a lot of cases now being reported, while earlier they were not being reported. The National AIDS Control Organisation has worked with communities that at one time in history fell onto the other side of the law. It has built models that have worked and are being replicated around India,” said Shree Alok Saxena, the Joint Secretary of the National AIDS Control Organisation.
Marietou Satin, Deputy Director of USAID, India, said, “Excluding any section of society is not only a moral evil, but it also impacts a country as a whole. You are denying a large population from being productive members of society. By including them, you are also investing in your economy. They have a right to contribute. For that, people need access to jobs and safety in the workplace.”
The meeting also saw the establishment of an LGBTI taskforce to provide strategic advice to UNAIDS and the United Nations Development Programme in India on current and emerging LGBTI issues in India, and on policy, programmes and services to address those issues.
The participants noted the need end discrimination, sensitize political leaders and policy-makers and ensure that the LGBTI community has access to all services, including health and education, and employment.
Region/country







Feature Story
Leveraging technology and innovation to end AIDS and tuberculosis
24 May 2019
24 May 2019 24 May 2019Leaders from both the private and public sectors have called for fresh investment models for new technologies and the smarter roll-out of innovations to end AIDS and tuberculosis by 2030.
The plea was made by panellists taking part in a debate at the Health Innovation Exchange, a three-day event organized by UNAIDS and held between 21 and 23 May on the sidelines of the World Health Assembly in Geneva, Switzerland.
Speaking at the event, the Executive Director of the Stop TB Partnership, Lucica Ditiu, said new approaches are vital in order to make faster progress in the response to the epidemics.
“We will not achieve our targets of ending AIDS and tuberculosis by doing things as we have always done them in the past,” she said. “Products must be developed with the patient in mind and we must work with developers to help them gather evidence that their innovations work in order to shorten the timeline from validation to implementation.”
Roland Göhde, chair of the German Healthcare Partnership, a joint venture of the Government of Germany and the Federation of German Industries, said there was an urgent need for greater synergies right along the chain of development and innovation. “The private sector needs to be systemically involved by other sectors. We need to bundle and conflate the different expertise of the involved sectors to get rid of fragmentation.”
Mr Göhde also underlined the importance of training in new technologies. He described how the German Healthcare Partnership had facilitated the training of laboratory workers in Burkina Faso in new haematology technologies as well as the training of biomedical engineers in Kenya and Senegal.
Jenifer Healy from USAID reminded the audience that the World Health Organization had estimated that the cost of achieving the Sustainable Development Goals health targets was an initial US$ 134 billion annually in 2017, rising to US$ 371 billion by 2030.
“While we have made great progress in global health, including in reducing the impact of AIDS, the funding gap for new investments will triple by 2030,” she said.
The Global Head of Public Health at Johnson & Johnson, Jaak Peeters, also underlined the importance of supporting the best science possible for global health, a more rapid implementation of best practice innovation and the fullest embrace of public–private collaboration.
In his comments, the Director-General of the Ghana Health Service, Anthony Nsiah-Asare, said that political commitment was required to ensure that innovation was deployed to deliver smarter, more efficient and high-quality services to the people most in need.
More information on

, an organization that works with male sex workers in Malawi. When Mr Mitha speaks of change, he does so with the qu")
Feature Story
“Be the change”: creating a voice for male sex workers in Malawi
27 May 2019
27 May 2019 27 May 2019“If I want to see the change, I need to be the change,” said Aniz Mitha, the Executive Director of Community Health Rights Advocacy (CHeRA), an organization that works with male sex workers in Malawi. When Mr Mitha speaks of change, he does so with the quiet and unwavering authority of someone who knows what he is talking about.
From a conservative Muslim family in Malawi, Mr Mitha was thrown out of the house at a young age when his parents found out that he was gay. With nowhere to go and no means to support himself, he fled to Johannesburg, South Africa, where he spent many years as a sex worker. “For me, I was looking to survive; I wasn’t thinking about my health,” he said.
When he became ill, he took an HIV test, and he learned that he was living with HIV. Being an illegal immigrant, he couldn’t access health-care services in South Africa. He returned to Malawi, where he began HIV treatment and started CHeRA. “I thought: how can I help others not go through the same experience that I did?” he said.
CHeRA raises awareness and builds the capacity of male sex workers on HIV prevention and treatment, sexual and reproductive health and rights, economic empowerment, psychosocial support and access to justice. Through a UNAIDS funding arrangement, it recently reached more than 250 male sex workers in three priority districts in Malawi, distributed more than 30 000 condoms and lubricant and linked six male sex workers living with HIV to care and treatment. In another programme funded by the Global Fund to Fight AIDS, Tuberculosis and Malaria, the organization has trained 50 peer educators and distributed more than 6000 condoms and condom-compatible lubricant.
Mr Mitha is keenly aware of the many challenges that face male sex workers, having faced them himself. “In Malawi, sex work is not recognized as work, so there are no laws to protect sex workers. Also, most of our male sex workers are gay men or men who have sex with men, so they live in fear of arrest because homosexuality is illegal in Malawi,” he said.
Stigma and discrimination is institutional, he said. “Male sex workers are not recognized as a key population in the HIV response in Malawi, so we are not prioritized in government plans. And negative attitudes from health-care workers push us away from care.”
“Say I am being abused or beaten and I go to a police station,” continues Mr Mitha, “I will get questions like “Why you are dressed like this or why do you speak like this?” The abuse is institutionalized. It pushes us away, so even in terms of health care, we go to private hospitals where we pay money even if we don’t have money.”
CHeRA is now registered as a nongovernmental organization. Although started in 2016, it was only registered in 2017 after UNAIDS played a pivotal role in amending provisions in the Malawi HIV and AIDS Management Control Act of 2018 that criminalized or discriminated against certain groups, such as sex workers. This paved the way for organizations of lesbian, gay, bisexual, transgender and intersex people and sex workers to be registered.
Like many people who serve others, his work has spilled over into his private life. Knowing what it feels like to be disowned by one’s family, Mr Mitha gives shelter to people who have nowhere else to go, who stay as long as it takes until they can look after themselves.
He has built an unshakeable sense of self, family and community through his work and his life. “I am living openly with HIV and as a gay person; I am a role model to so many. They see that it is possible. I see a lot more people like me opening up and living openly as gay and with HIV,” he said.
Mr Mitha wants to grow CHeRA into an organization that is a strong advocate for equitable access to health care for male sex workers.
“We need more financial support to expand the work we do,” he said. “We provide access to HIV prevention information and services to a population that is being left behind. It is making a difference. When you are working as a community organization, it means what affects my community affects me too,” he said.
Related information
Region/country



Feature Story
First Lady of Kenya visits UNAIDS to highlight Beyond Zero
22 May 2019
22 May 2019 22 May 2019The First Lady of Kenya, Margaret Kenyatta, visited UNAIDS headquarters in Geneva, Switzerland, on 21 May to talk about her Beyond Zero initiative to improve maternal and child health and to reduce the impact of HIV in the country. During her visit, Ms Kenyatta met UNAIDS Executive Director, a.i., Gunilla Carlsson and addressed staff at a town hall meeting.
Since its launch in January 2014, the Beyond Zero initiative has transformed the lives of thousands of women and children across Kenya, mobilizing resources and forging new partnerships to improve health outcomes, with a special emphasis on reducing maternal and child deaths and preventing new HIV infections.
Beyond Zero has delivered more than 50 mobile clinics to every county in Kenya. The clinics have resulted in increased access to and uptake of health-care services. The initiative has also made a significant contribution to the progress made in the country’s AIDS response, with new HIV infections among children down from about 13 000 in 2013 to 8000 in 2017.
With the launch of the Beyond Zero Medical Safari in 2018, the focus is on providing free health care and surgical services, including fistula surgeries, to Kenyans in remoter parts of the country. There is also a strong commitment to increase the social inclusion of children living with disabilities and to engage with adolescents to reduce the risk of HIV infection.
Ms Kenyatta told UNAIDS staff that the response to HIV had to be continued with renewed vigour.
“We cannot leave the battlefield just yet,” she said. “We must recommit ourselves to ending AIDS by 2030 so that in the years to come, when AIDS will be spoken of as a thing of the past, we shall remember the roles we played, however big or small.”
Ms Carlsson thanked Ms Kenyatta for her continued support for the response to HIV.
“The First Lady is an incredible advocate for maternal and child health. She is a champion for issues that are close to our hearts. The Beyond Zero initiative is transforming the lives of women and children across Kenya.”
Accompanying Ms Kenyatta on her visit to UNAIDS were Kenya’s Cabinet Secretary for Health, Sicily Kariuki, the Chair of the National AIDS Control Council, Nduku Kilonzo, and Kenya’s Ambassador to the United Nations in Geneva, Cleopa Mailu.