Tuberculosis TB

Publications





Documents
UNAIDS Executive Director meets with Brazilian Government and civil society
UNAIDS Executive Director Mr Michel Sidibé held a series of meetings with Government officials and civil society groups in Rio de Janeiro and Brasilia during his official visit to Brazil.
Related
 The critical impact of the PEPFAR funding freeze for HIV across Latin America and the Caribbean
The critical impact of the PEPFAR funding freeze for HIV across Latin America and the Caribbean
19 de febrero de 2025
 Peru approves groundbreaking law to extend health coverage for migrants with HIV and TB
Peru approves groundbreaking law to extend health coverage for migrants with HIV and TB
21 de octubre de 2024
2024 global AIDS report — The Urgency of Now: AIDS at a Crossroads
22 de julio de 2024
 UNAIDS commends Mexico's ban on conversion therapy
UNAIDS commends Mexico's ban on conversion therapy
12 de junio de 2024
 Guayaquil joins the worldwide group of cities committed to ending the HIV epidemic
Guayaquil joins the worldwide group of cities committed to ending the HIV epidemic
15 de marzo de 2024
 Seeking justice for HIV-related discrimination in the workplace in Guatemala
Seeking justice for HIV-related discrimination in the workplace in Guatemala
18 de diciembre de 2023
 Responding to gender-based violence through sorority and information
Responding to gender-based violence through sorority and information
15 de diciembre de 2023
 Visita conjunta de cuatro días de socios de la cooperación internacional en VIH a Honduras finaliza con conmemoración del Día Mundial del SIDA en Tegucigalpa
Visita conjunta de cuatro días de socios de la cooperación internacional en VIH a Honduras finaliza con conmemoración del Día Mundial del SIDA en Tegucigalpa
04 de diciembre de 2023
 Ahead of World AIDS Day UNAIDS is calling for urgent support to Let Communities Lead in the fight to end AIDS
Ahead of World AIDS Day UNAIDS is calling for urgent support to Let Communities Lead in the fight to end AIDS
30 de noviembre de 2023
Summary — Let Communities Lead — UNAIDS World AIDS Day report 2023
28 de noviembre de 2023
Documents
UNAIDS Executive Director, Michel Sidbé visits Brazil
UNAIDS Executive Director Mr Michel Sidibé visited the Rio de Janeiro based Viva Cazuza Society on 26 March, a non-profit organization that provides a home for 20 children and adolescents, aged 2 to 16, who are living with HIV.
Related
The critical impact of the PEPFAR funding freeze for HIV across Latin America and the Caribbean
19 de febrero de 2025
Peru approves groundbreaking law to extend health coverage for migrants with HIV and TB
21 de octubre de 2024
2024 global AIDS report — The Urgency of Now: AIDS at a Crossroads
22 de julio de 2024
UNAIDS commends Mexico's ban on conversion therapy
12 de junio de 2024
Guayaquil joins the worldwide group of cities committed to ending the HIV epidemic
15 de marzo de 2024
Seeking justice for HIV-related discrimination in the workplace in Guatemala
18 de diciembre de 2023
Responding to gender-based violence through sorority and information
15 de diciembre de 2023
Visita conjunta de cuatro días de socios de la cooperación internacional en VIH a Honduras finaliza con conmemoración del Día Mundial del SIDA en Tegucigalpa
04 de diciembre de 2023
Ahead of World AIDS Day UNAIDS is calling for urgent support to Let Communities Lead in the fight to end AIDS
30 de noviembre de 2023
Summary — Let Communities Lead — UNAIDS World AIDS Day report 2023
28 de noviembre de 2023
Documents
UNAIDS Executive Director Michel Sidibé attends 3rd Stop TB Partners Forum, Rio de Janeiro
The Executive Director of UNAIDS, Mr Michel Sidibé is in Brazil this week to attend the 3rd TB Partners Forum. Earlier today in Rio de Janeiro, Mr Sidibé also joined the international launch of the World Health Organization’s annual report on global TB control.
Related
The critical impact of the PEPFAR funding freeze for HIV across Latin America and the Caribbean
19 de febrero de 2025
Peru approves groundbreaking law to extend health coverage for migrants with HIV and TB
21 de octubre de 2024
2024 global AIDS report — The Urgency of Now: AIDS at a Crossroads
22 de julio de 2024
UNAIDS commends Mexico's ban on conversion therapy
12 de junio de 2024
Guayaquil joins the worldwide group of cities committed to ending the HIV epidemic
15 de marzo de 2024
Seeking justice for HIV-related discrimination in the workplace in Guatemala
18 de diciembre de 2023
Responding to gender-based violence through sorority and information
15 de diciembre de 2023
Visita conjunta de cuatro días de socios de la cooperación internacional en VIH a Honduras finaliza con conmemoración del Día Mundial del SIDA en Tegucigalpa
04 de diciembre de 2023
 UNAIDS welcomes new decision in Colombia allowing more affordable access to quality HIV medicines
UNAIDS welcomes new decision in Colombia allowing more affordable access to quality HIV medicines
04 de octubre de 2023
 Addressing violence against women sex workers in Peru
Addressing violence against women sex workers in Peru
27 de julio de 2023
Documents
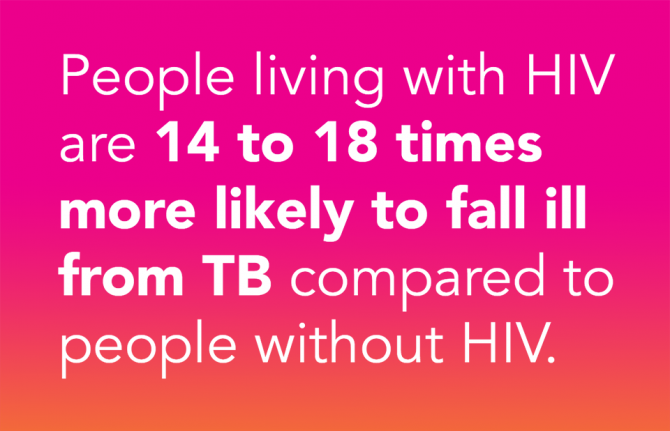
Tuberculosis and HIV: the dual epidemic
Up to half of all deaths in people living with HIV are caused by tuberculosis - Yet TB is both preventable and curable.
Related
2024 global AIDS report — The Urgency of Now: AIDS at a Crossroads
22 de julio de 2024
 UNAIDS Executive Director Message on World TB Day – Yes, we shall and we can end TB among people living with HIV!
UNAIDS Executive Director Message on World TB Day – Yes, we shall and we can end TB among people living with HIV!
24 de marzo de 2023
 Impact of COVID-19 hits hard as TB deaths among people living with HIV rise for the first time since 2006
Impact of COVID-19 hits hard as TB deaths among people living with HIV rise for the first time since 2006
23 de marzo de 2022
 TB disease and deaths declining among people living with HIV, but there have been some reversals due to the COVID-19 pandemic
TB disease and deaths declining among people living with HIV, but there have been some reversals due to the COVID-19 pandemic
23 de marzo de 2022
40 years of the AIDS response
08 de junio de 2021
 Tuberculosis deaths among people living with HIV are declining globally, but worrying gaps in TB care persist
Tuberculosis deaths among people living with HIV are declining globally, but worrying gaps in TB care persist
24 de marzo de 2021
 Huge gaps in TB care for people living with HIV in some countries
Huge gaps in TB care for people living with HIV in some countries
24 de marzo de 2021
 Tuberculosis testing gap among people living with HIV is narrowing
Tuberculosis testing gap among people living with HIV is narrowing
15 de febrero de 2021
 51st Union World Conference on Lung Health opens today as gains in reducing TB deaths risk being set back by COVID-19
51st Union World Conference on Lung Health opens today as gains in reducing TB deaths risk being set back by COVID-19
20 de octubre de 2020
 Innovative and people-empowered approaches to end TB deaths
Innovative and people-empowered approaches to end TB deaths
25 de marzo de 2020

Feature Story
El informe de la OMS señala un aumento en el número de casos de tuberculosis farmacorresistente
19 Marzo 2010
19 Marzo 2010 19 Marzo 2010
Por primera vez, el informe anual de la OMS incluye una evaluación del progreso que han experimentado algunos países en lo que concierne a la diagnosis y al tratamiento de la tuberculosis multirresistente.
Un cuarto de las personas que viven con tuberculosis en ciertas regiones del mundo ya no pueden recibir un tratamiento basado en la farmacoterapia estándar. Esta es la dura realidad que se ha puesto de manifiesto en el nuevo informe de la Organización Mundial de la Salud, donde se calcula que, en 2008, 440.000 personas padecían tuberculosis multirresistente (MDR-TB), y que un tercio de las cuales falleció a causa de la enfermedad.
El documento La tuberculosis multirresistente y extremadamente farmacorresistente (M/XDR-TB): Informe anual sobre la vigilancia y la respuesta ofrece información acerca de 114 países diferentes, y hace hincapié en el hecho de que casi la mitad de los casos de MDR-TB se dan en China y en la India. Por otro lado, se calcula que, en África, han aparecido aproximadamente 69.000 nuevos casos.
En dicho informe, también se estudia la relación existente entre el VIH y la MDR-TB, y se indica que, en ciertos lugares, tales como los hospitales, se han registrado numerosos casos de tuberculosis farmacorresistente entre las personas que viven con el VIH. Asimismo, el informe apunta que, en tres países de Europa del este (Estonia, Letonia y la República de Moldova), se ha descubierto que los pacientes que sufren tuberculosis y VIH están expuestos a un mayor riesgo de padecer tuberculosis multirresistente en comparación con los pacientes de tuberculosis que no han contraído la infección por el VIH. Los estudios llevados a cabo en Lituania, Ucrania y Mozambique arrojan resultados similares. Con todo, es necesario realizar más investigaciones para determinar si dichos datos podrían ser aplicables a nivel mundial, pues el informe establece que todavía no se ha recibido información alguna de los países en los que se registran los índices de mayor prevalencia del VIH.
Según los datos de ONUSIDA, las personas VIH-positivas son especialmente vulnerables al impacto de la tuberculosis simple y de la tuberculosis multirresistente, dado que están expuestas a un mayor riesgo de contraer la enfermedad, de sufrir los graves efectos secundarios derivados de la misma e incluso de fallecer a causa de la nueva infección. El VIH y la tuberculosis están tan estrechamente ligados que a menudo se hace referencia a ellos como "coepidemias" o "dobles epidemias". Por ello, para poder ofrecer una respuesta adecuada para ambas y evitar la propagación de la farmacorresistencia, es preciso que los servicios totalmente integrados para el VIH y la tuberculosis sean una prioridad en los programas de tuberculosis y VIH.
Evitar que las personas que viven con el VIH fallezcan a causa de la tuberculosis es una de las nueve áreas de prioridad del Marco de resultados de ONUSIDA 2009-11.

Según el informe de la OMS, solo a aproximadamente un 7% de todos los pacientes que sufren tuberculosis multirresistente se les ha diagnosticado la enfermedad. Photo: OMS/D.Orr
Por primera vez, el informe anual de la OMS incluye una evaluación del progreso que han experimentado algunos países en lo que concierne a la diagnosis y al tratamiento de la tuberculosis multirresistente, seis de los cuales han constituido el centro del estudio. Bangladesh es uno de los pocos países en desarrollo que está llevando a cabo un continuo seguimiento de los casos de tuberculosis que ya habían sido tratados en determinadas áreas. China ha presentado los resultados de su primera encuesta realizada en materia de farmacorresistencia; Etiopía, por su parte, fue uno de los primeros países en poner en práctica las primeras pruebas moleculares de laboratorio rápidas. Nepal y Rumanía cuentan con programas de tratamiento específicos para la MDR-TB eficaces, y Sudáfrica ha llevado a cabo cambios en sus políticas, a fin de mejorar la gestión y la atención brindada a todos aquellos que viven con la enfermedad.
Si bien se han experimentado grandes logros en algunos países, los avances conseguidos a nivel mundial en lo que se refiere al control de la tuberculosis multirresistente todavía siguen siendo escasos. Según el informe de la OMS, solo a aproximadamente un 7% de todos los pacientes que sufren tuberculosis multirresistente se les ha diagnosticado la enfermedad.
Otra de las principales preocupaciones en torno a este tema es el coste extremadamente elevado del tratamiento necesario para esta forma de tuberculosis. Solo el precio de los medicamentos es entre 50 y 200 veces mayor que el del tratamiento que debe seguir un paciente que sufre tuberculosis sin ningún tipo de resistencia a los fármacos. No obstante, la OMS afirma que se ha constatado que el tratamiento de la MDR-TB sí es rentable.
Finalmente, cabe destacar que, según lo indicado en el informe, es extremadamente necesario conseguir medicamentos eficaces para reducir el tratamiento a un periodo de tiempo inferior a dos años, así como lograr una mejora de las instalaciones de los laboratorios y conseguir un acceso rápido a los servicios de diagnosis y tratamiento. La OMS ha emprendido un proyecto de cinco años, cuyo objetivo consiste en reforzar la eficacia de los laboratorios de tuberculosis por medio de la realización de pruebas rápidas en 30 países diferentes. Asimismo, la OMS está trabajando conjuntamente con un gran número de organizaciones, a fin de aumentar las posibilidades de acceso al tratamiento, de manera que se puedan salvar más vidas.
Nota: La tuberculosis multirresistente (MDR-TB) se define por la resistencia del bacilo que provoca la enfermedad a, como mínimo, la rifampicina y la isoniazida, los dos antituberculosos más potentes. La tuberculosis extremadamente farmacorresistente (XDR TB), por su parte, se define como la MDR-TB que también ofrece resistencia a, como mínimo, dos de las tres clases de los antituberculosos de segunda línea.
El informe de la OMS señala un aumento en el núme
Políticas y orientaciones:
Tuberculosis - Políticas técnicas de ONUSIDA
Información relacionada:
Tuberculosis y VIH
Coinfección
Copatrocinadores:
Organización Mundial de la Salud
Asociados:
Iniciativa Alto a la tuberculosis (en inglés)
Reportajes:
Llamamiento a una acción global para hacer frente a la amenaza de la tuberculosis resistente a los medicamentos (3 de abril de 2009)
Llamamiento para la plena capitalización del Fondo Mundial (31 de marzo de 2009)
El Director ejecutivo de ONUSIDA se reúne con directores de programas de tuberculosis y representantes de la sociedad civil (26 de marzo de 2009)
Urge ampliar los sistemas de detección integral de la TB y el VIH para abordar ambas epidemias interrelacionadas (24 de marzo de 2009)
Las muertes por tuberculosis aumentan entre las personas que viven con el VIH (17 de marzo de 2008)
La tuberculosis multirresistente es más frecuente en personas que viven con el VIH (28 de febrero de 2008)
Publicaciones:
La tuberculosis multirresistente y extremadamente farmacorresistente (M/XDR-TB): Informe anual sobre la vigilancia y la respuesta (pdf, 850 Kb) (en inglés)
Related
 Virtual course on HIV, gender and human rights: empowering medical teachers in Guatemala
Virtual course on HIV, gender and human rights: empowering medical teachers in Guatemala
18 de mayo de 2023
 United for ending cervical cancer, HIV and inequities for women and girls
United for ending cervical cancer, HIV and inequities for women and girls
17 de noviembre de 2022

Feature Story
New data shows progress in addressing TB/HIV
08 Diciembre 2009
08 Diciembre 2009 08 Diciembre 2009
Some 36 million people have been cured of tuberculosis (TB) over the past 15 years through a rigorous approach to treatment endorsed by the World Health Organization (WHO). New data, released by WHO, also indicate that up to 8 million TB deaths have been averted, confirming the Stop TB Strategy as the most cost-effective approach in the fight against TB.
The WHO update also shows continued progress on addressing the lethal combination of TB and HIV. Between 2007 and 2008, 1.4 million TB patients were tested for HIV, an increase of 200, 000. Of those who tested HIV positive, one-third benefited from life-saving HIV anti-retroviral therapy (ART) and two-thirds were enrolled on co-trimoxazole prophylaxis to prevent the risk of fatal bacterial infections. In addition, screening for tuberculosis and access to isoniazid preventive therapy for TB among people living with HIV more than doubled, although the total number is still far short of what it should be.
"Fifteen years of TB investments are bringing visible results in terms of human lives saved. Together, national programmes, WHO, UNAIDS, the Global Fund and other partners have helped save millions of lives from TB," said Dr Mario Raviglione, Director of WHO's Stop TB Department. "But the current pace of progress is far from sufficient to decisively target our goal of TB elimination."
The WHO Stop TB Strategy has five elements: political commitment with increased and sustained financing, case detection through quality-assured bacteriology, standardized treatment with supervision and patient support, an effective drug supply and management system, monitoring and evaluation system and impact measurement.
Data from the latest 12 month period now show that the highest ever number of infectious patients - 2.3 million people - were cured. With 87% of treated patients cured, the 85% global target was exceeded for the first time since it was established in 1991. Furthermore, a total of 53 countries surpassed this treatment milestone.
Fifteen years of TB investments are bringing visible results in terms of human lives saved. Together, national programmes, WHO, UNAIDS, the Global Fund and other partners have helped save millions of lives from TB.
Dr Mario Raviglione, Director of WHO's Stop TB Department
Although more and more patients are being cured, there are millions who are being let down because they are unable to access high-quality care. TB remains second only to AIDS in terms of the number of people it kills. In 2008, 1.8 million people died from TB including half a million deaths in HIV related illness–many of them because they were not enrolled on ART.
A persistent challenge that is largely left unchecked in many parts of the world is multidrug-resistant TB (MDR-TB) and its even more dangerous form, extensively drug-resistant TB (XDR-TB). Of the estimated half a million MDR-TB cases occurring per year, almost 30 000 were officially reported and 6 000 were known to be treated according to WHO international standards in 2008. A major expansion of services is currently in an early and difficult phase but almost 29 000 people are expected to be treated in 2010.
Of the estimated 9.4 million TB cases in 2008 (including 1.4 million TB/HIV cases), 3.6 million cases occurred among women.
"Half a million women died from TB last year. It is a disease that destroys lives, damages families and stifles development," said Dr Mario Raviglione. "Without help to fill the US$ 2 billion funding gap for TB care and control in 2010, the most vulnerable people will continue to miss the benefits so many others have seen."
The new report provides the most accurate information on the global burden of tuberculosis. It also features updates about the work of the Global Laboratory Initiative, the WHO Global Task Force on TB Impact Measurement, and describes the success of a new initiative in 2009 in which global TB data collection went online.
New data shows progress in addressing TB/HIV
Cosponsors:
Partners:
Stop TB Partnership
The Global Fund
Feature stories:
UNAIDS Executive Director meets with TB Programme Managers, TB civil society (26 March 2009)
Publications:
Global tuberculosis control: a short update to the 2009 report
Contact:
For further information, please contact:
Glenn Thomas,
Senior Communications Adviser, Stop TB Department,
WHO +41 79 509 0677,
E-mail: thomasg@who.int
All WHO information can be found at www.who.int
Related
Virtual course on HIV, gender and human rights: empowering medical teachers in Guatemala
18 de mayo de 2023
United for ending cervical cancer, HIV and inequities for women and girls
17 de noviembre de 2022
Feature Story
La tuberculosis multirresistente es más frecuente en personas que viven con el VIH
28 Febrero 2008
28 Febrero 2008 28 Febrero 2008
La Organización Mundial de la Salud (OMS) presentó el 26 de febrero su cuarto informe anual. Este se centra en la tuberculosis farmacorresistente y señala que la tuberculosis multirresistente es casi el doble de frecuente en personas con tuberculosis (TB) que viven con el VIH que en el caso de personas que paceden tuberculosis y que, por el contrario, no viven con el virus.
El informe muestra los resultados del mayor estudio sobre la tuberculosis farmacorresistente realizado hasta la fecha, con datos recogidos entre 2002 y 2006 de 90000 personas que viven con tuberculosis en 81 países. En él se muestran los índices más elevados de tuberculosis multirresistente que se han registrado hasta la fecha, con casi medio millón de casos nuevos en el mundo al año (alrededor del 5% de los 9 millones de casos nuevos de tuberculosis). Igualmente comprobó que la tuberculosis extremadamente resistente**, un tipo de esta enfermedad respiratoria que prácticamente no se puede tratar, se ha registrado en 45 países.
También sigue sin conocerse la verdadera magnitud del problema en algunos lugares aislados del mundo. Solamente seis países de África, la región con mayor incidencia de tuberculosis del mundo, pudieron proporcionar datos sobre la resistencia a los fármacos para el informe y ninguno de ellos pudo proporcionarlos en relación a las personas que viven con el VIH. Otros países de la región no pudieron realizar estudios porque carecen de los medios y del personal cualificado que se requieren para identificar la tuberculosis resistente.
“Este informe confirma la gran amenaza que supone la tuberculosis farmacorresistente para la gente que vive con el VIH”, dijo Alasdair Reid, consejero del VIH y la tuberculosis en ONUSIDA. “ONUSIDA junto con la OMS y nuestros socios internacionales coopera en programas de tuberculosis y VIH en países de todo el mundo para asegurar que su colaboración es más estrecha, y así, prevenir el desarrollo y la propagación de la tuberculosis farmacorresistente entre personas que viven con el VIH. Todo gracias a un mejor diagnóstico y tratamiento de la tuberculosis en estas personas y a un mejor control de dicha infección en entornos de asistencia del VIH y en comunidades afectadas por este virus”.
Según las estimaciones de la OMS, se necesitan US$ 4800 millones para el control global de la tuberculosis en países de renta baja y media en 2008 y US$ 1000l millones para hacer frente a la tuberculosis farmacorresistente. Actualmente hay un déficit de financiación de US$ 2500 y otro de US$ 500 millones que irían destinados contra la tuberculosis resistente.
NOTA A LOS REDACTORES:
* La bacteria que causa la tuberculosis se vuelve resistente cuando a las personas que la padecen no se les proporciona un tratamiento o no finalizan el mismo. La tuberculosis farmacorresistente, al igual que la tuberculosis sensible a los fármacos, también se transmite de una persona que la padece a una persona sana a través del aire. Pero al contrario que ésta, la tuberculosis multirresistente no responde al tratamiento convencional de seis meses con medicamentos de primera línea (por ejemplo a la isoniazida y a la rifampicina). El tratamiento puede durar dos años con medicamentos que son 100 veces más caros que los de primera línea.
** La tuberculosis extremadamente resistente es un tipo de tuberculosis causada por bacterias resistentes a prácticamente todos los medicamentos más efectivos (además de aquellos de la tuberculosis multirresistente, a cualquier fluoroquinolona y a todos los medicamentos inyectables de segunda línea: amicacina, kanamicina y capreomicina).
*** En África Subsahariana, el VIH está provocando una propagación catastrófica de la tuberculosis, que es una causa principal de mortalidad para la gente que vive con el VIH. Las tuberculosis multirresistente y extremadamente resistente son potencialmente mortales para la gente que vive con el VIH (algunos estudios muestran índices de mortalidad superiores al 90%). Por eso, la tuberculosis farmacorresistente constituye la principal amenaza para la eficacia de los tratamientos contra la tuberculosis y para los programas de tratamiento antirretrovíricos.
La tuberculosis multirresistente es más frecuente
Copatrocinadores:
OMS (en inglés)
Enlaces relacionados:
Alianza contra la tuberculosis farmacorresistente en el mundo (en inglés)
Publicaciones:
Resistencia a medicamentos anti-tuberculosis en el mundo (pdf, 2.4 Mb) (en inglés)
Related
Virtual course on HIV, gender and human rights: empowering medical teachers in Guatemala
18 de mayo de 2023
United for ending cervical cancer, HIV and inequities for women and girls
17 de noviembre de 2022
Feature Story
Joining forces to tackle TB and HIV
24 Noviembre 2006
24 Noviembre 2006 24 Noviembre 2006 Photo credit : WHO
Photo credit : WHOTuberculosis (TB) is one of the biggest killers of people living with HIV and at least one third of the 39.5 million people estimated to be living with HIV around the world are likely to be infected with the TB bacteria. As a result of chronically poor investment in global TB control a new strain of TB is emerging that has become resistant to most of the available anti-tuberculosis drugs. Known as extensively drug resistant TB (XDR TB) this strain has serious implications for people living with HIV as it is almost untreatable in many of the countries where it is occurring leading to very high death rates. WHO and UNAIDS, together with other actors working on TB and HIV issues are stepping up action to stop the spread of TB and this deadly new strain.
TB is an infection which usually affects the lungs and is spread, like the common cold, through the air from an infectious person coughing, sneezing or even speaking. One third of the world’s population is infected with TB but only 5-10% of people who are infected with TB actually develop TB disease during their lifetimes. However, co-infection with HIV makes TB disease much more likely and one in ten people infected with TB who also have HIV will develop TB disease each year.
TB is treatable and can usually be cured in people living with HIV, however some strains of TB bacteria have now acquired resistance to one or more of the antibiotics commonly used to treat them; these are known as drug-resistant strains. Treatment for these infections is much longer and much more expensive. The recent outbreaks of tuberculosis that is resistant to almost all of the available TB drugs are giving serious cause for concern as this extensively drug resistant strain (XDR TB) is virtually untreatable when it occurs in people living with HIV and has a very high death rate.
UNAIDS has been following the developments closely. “We need to rapidly ensure prompt diagnosis and effective treatment of TB for people living with HIV in order to prevent drug resistance from developing and spreading,” said UNAIDS’ HIV/TB advisor, Alasdair Reid.
TB drug resistance arises mainly because of inadequate TB control, poor patient or clinician adherence to standard TB treatment regimens, poor quality drugs or inadequate drug supplies. People living with HIV are particularly vulnerable to developing drug-resistant TB because of their increased susceptibility to infection and progression to active TB.
At the 37th Union World Conference on Lung Health held in Paris in November 2006, the interaction between TB and HIV and the threat of extensively drug resistant TB featured prominently in the agenda. The serious implications of the new strain of XDR TB for people living with HIV were highlighted at a special plenary session held during the conference. Dr Kevin De Cock, Director of WHO HIV/AIDS Department said, “The recent emergence of a cluster of cases in South Africa has demonstrated the high mortality that XDR TB can have when associated with HIV infection. Countries with a high prevalence of HIV have been responding quickly to draw up plans for managing and preventing drug-resistant TB and this is welcomed.”
Because of the serious threat that TB and especially XDR TB poses for people living with HIV, UNAIDS and the WHO HIV and TB departments are joining forces to encourage a coordinated and concerted global effort to control TB in people living with HIV.
WHO’s Global Task Force on XDR TB have recently published a report outlining measures needed to urgently combat extensively drug-resistant XDR TB. It follows the announcement by WHO and its partners that US$ 95 million will be required to implement the recommendations in the report, to address the threat of XDR-TB in 2007 in southern Africa. WHO have also released new guidelines on how to improve the diagnosis of TB in people living with HIV.
Links:
Access WHO new guidelines.
Frequently asked questions about Tuberculosis and HIV.
WHO TB
Stop TB partnership
Presentations from the Union meeting on XDR TB can be viewed through the Kaisernetworks link on the Union website.
International Union Against Tuberculosis and Lung Disease
Related
Virtual course on HIV, gender and human rights: empowering medical teachers in Guatemala
18 de mayo de 2023
United for ending cervical cancer, HIV and inequities for women and girls
17 de noviembre de 2022
Feature Story
New African resolve to combat AIDS, TB and Malaria
08 Mayo 2006
08 Mayo 2006 08 Mayo 2006
From right: Representative of UN Secretary General, Executive Director UNAIDS, Dr Peter Piot; President of Niger Republic, Mamodou Tandja and President Council of Senate Senegal, Mbaye-Jacques Diop on arrival for the opening session of the meeting of Heads of State and Government at the Special Summit of the African Union on HIV/AIDS, Tuberculosis and Malaria in Abuja
Photo: Sunday Aghaeze
African leaders and Heads of State recently met in Abuja, Nigeria at a Special Summit on HIV/AIDS, Tuberculosis and Malaria to address the challenges posed by the three diseases that kill an estimated four million Africans every year.
Organized by the African Union in collaboration with UN Agencies and other development partners, and at the invitation of Nigerian President Olusegun Obasanjo, the Special Summit adopted the Abuja Call for accelerated action towards Universal Access to AIDS, tuberculosis and malaria (ATM) services in Africa, and a resolution to achieve this by 2010. The delegates also adopted an African Common Position to be presented to the High Level Meeting on AIDS in June 2006.
In the Abuja Call, participants urged for intensified leadership at all levels; further commitments regarding human rights; increased mobilization of resources including negotiations for debt cancellation; and collective advocacy with multilateral and bilateral donors.
African leaders renewed their commitment to allocate 15% of their national budgets to health, and to incorporate health financing plans into national development plans.
“For the first time the political commitment exists to work towards Universal Access to HIV prevention, treatment and care, but getting this will require that once more we change gear and further accelerate the response to AIDS. We have no other options that will save entire societies”, said UNAIDS Executive Director Dr Peter Piot.
Nigerian President Olusegun Obasanjo commended African countries for the progress they had so far made in responding to AIDS, tuberculosis and malaria. The Nigerian leader called for the development of structures and systems guaranteeing better and more transparent utilization of funds, as well as for the development of strategies translating national level goals into community targets.

Press Conference after the closing of the Special Summit (left to right) Alpha Oumar Konaré, Chairperson of African Union Commission and former President of Mali; President Sassou-Nguesso of Republic of Congo, Chairman of the African Union; President Olusegun Obasanja of Nigeria, Host of the Special Summit and Alhaji Mamadou Tandja, President of Niger Republic
Photo: Sunday Aghaeze
Also speaking on the occasion, African Union Commission Chairperson, Prof. Alpha Konare, outlined measures Africa should adopt to successfully deliver AIDS, tuberculosis and malaria services. These include local production of essential medicines, greater mobilization of resources, more efficient utilization of resources, and ensuring access to the most vulnerable groups.
Sub-Saharan Africa has just over 10% of the world’s population, but is home to more than 60% of all people living with HIV - 25.8 million. In 2005, an estimated 3.2 million people in the region became newly infected, while 2.4 million adults and children died of AIDS. Among young people aged 15-24 years, an estimated 4.6% of women and 1.7% of men were living with HIV in 2005.
Related links
Read Statement of the UNAIDS Executive Director Dr Peter Piot at the Special Assembly of Heads of State and Government, Abuja, 4 May 2006
Photo gallery
3 April 2006
4 April 2006
Related
Peru approves groundbreaking law to extend health coverage for migrants with HIV and TB
21 de octubre de 2024
 Leave no one behind and that includes people who use drugs
Leave no one behind and that includes people who use drugs
04 de mayo de 2023
 Dangerous inequalities and overcoming them
Dangerous inequalities and overcoming them
18 de noviembre de 2022