Young people




Update
ACT!2015 at ECOSOC Youth Forum
10 February 2017
10 February 2017 10 February 2017Youth advocates from Bulgaria, Jamaica, Kenya, Mexico, the Philippines, Uganda and Zimbabwe represented ACT!2015—a youth-led social action initiative supported by UNAIDS, the International Planned Parenthood Federation and the PACT—at the United Nations Economic and Social Council (ECOSOC) Youth Forum’s 2017 meeting.
Held on 30 and 31 January in New York, United States of America, the Youth Forum focused on the role of youth in poverty eradication and promoting prosperity in a changing world. The annual forum provides a platform for young people to engage in meaningful conversations with United Nations Member States and to propose solutions to the world’s most pressing challenges.
ACT!2015’s youth-led, data-driven accountability was showcased in several breakout sessions that fostered in-depth discussions on the progress achieved so far on specific Sustainable Development Goals (SDGs), including SDG 3 (healthy lives and promoting well-being) and SDG 5 (gender equality).
The forum served as a platform for three youth advocates from ACT!2015 to strengthen their collaboration with representatives of Kenya and Zimbabwe, which will undergo voluntary reviews of their progress on the Sustainable Development Goals at the upcoming High-Level Political Forum on Sustainable Development, to be held in July.
In the months leading up to the High-Level Political Forum on Sustainable Development, ACT!2015 national youth alliances will gather their own evidence around policy issues identified as key barriers to accessing HIV and sexual and reproductive health services. This evidence will be translated into national advocacy road maps aimed at starting a national process for the review and reform of restrictive laws and policies.
Quotes
“We all have a role to play and a responsibility to uphold our commitments with the Sustainable Development Goals and the United Nations Political Declaration on Ending AIDS. The United Nations Economic and Social Council Youth Forum has been a testament to young people’s commitment and unbreakable aspiration to achieve the targets and goals.”
“I participated in discussions surrounding women and girls and the broader topic of gender equality and how transgender women, men and gender nonconforming persons fit into the conversation. This experience has taught me the importance of networking and building strong relationships as well as sharing best practices, which is key in successfully implementing the Sustainable Development Goals.”
“ACT!2015 is proudly youth-led and our guiding principle is that young people have the right to participate in decision-making and to access health education and services that meet their needs. This forum has been a great opportunity for us to show that we are not going to stop pushing for youth engagement and for young people’s voices to be heard and listened to by governments.”
Related information






Update
International conference in Thailand addresses health of vulnerable populations
03 February 2017
03 February 2017 03 February 2017The Prince Mahidol Award Conference brought together international leaders in public health to discuss high-priority health issues in Bangkok, Thailand. The 10th annual gathering was held under the theme “Addressing the health of vulnerable populations for an inclusive society” and took place from 29 January to 3 February.
Her Royal Highness Princess Maha Chakri Sirindhorn attended the opening session, which included a keynote address from Nobel Laureate Amartya Sen, of Harvard University, who spoke about how living in a sharply unequal society affects health.
UNAIDS and the Global Fund to Fight AIDS, Tuberculosis and Malaria organized a session called From Exclusion to Leadership: Learning from the AIDS Response. The session explored how knowledge from the response to HIV could be used in addressing vulnerability, marginalization and social exclusion at the global, regional and national levels. It looked at lessons and approaches that are transferable to the broader health agenda.
Another session co-organized by UNAIDS and the World Health Organization was entitled Discrimination in Health Care—Determinants and Consequences. It examined how discrimination leads to poor health outcomes, leaving people who are stigmatized even more vulnerable to ill-health and its consequences.
Quotes
“To neglect the health of some while others enjoy health care is a sure way to perpetuate social injustice.”
“We can’t end this epidemic unless we become better human beings. We have to look outward, forward and with hope, instead of inward with hate.”
“We have three strategies to ending AIDS: prevention, prevention and prevention. We must turn off the tap.”
“It’s not just about pills; it’s about policies, laws, criminalization, women, girls and adolescents.”
“Now, we must legalize the community-led health service model, led by key populations. We must accredit the community health workers.”
“Vulnerable people are not asking for more rights; they are just asking for the same rights that all of us enjoy.”
Resources
Region/country
Related
 Status of HIV Programmes in Indonesia
Status of HIV Programmes in Indonesia
24 February 2025
Documents
Ending the AIDS epidemic for adolescents, with adolescents
31 December 2016
A practical guide to meaningfully engage adolescents in the AIDS response
Related

UNAIDS data 2024
02 December 2024
Take the rights path to end AIDS — World AIDS Day report 2024
26 November 2024
 The AIDS response is recognized as a beacon of hope and guide for revitalizing multilateralism at the 79th UN General Assembly
The AIDS response is recognized as a beacon of hope and guide for revitalizing multilateralism at the 79th UN General Assembly
27 September 2024
 Young people living with HIV urge world leaders to partner with them in the AIDS response
Young people living with HIV urge world leaders to partner with them in the AIDS response
19 September 2024




Feature Story
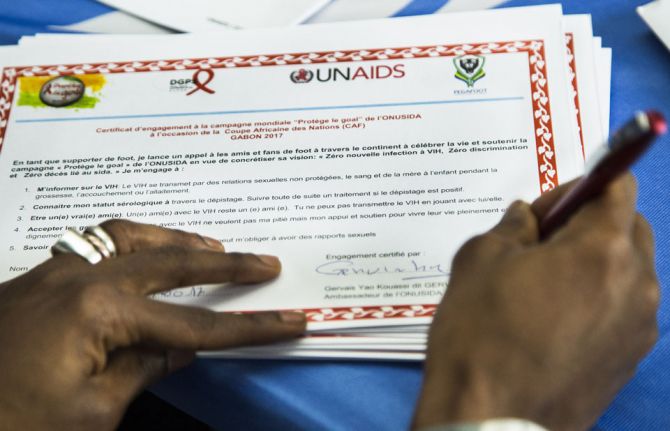
Gervinho meets young people affected by HIV in Gabon ahead of CAN 2017
19 January 2017
19 January 2017 19 January 2017Travelling to Gabon to attend the Africa Cup of Nations (CAN 2017), Gervais Yao Kouassi (Gervinho), UNAIDS Special Ambassador for Youth and China–Africa Collaboration, visited the UNAIDS office in Libreville, Gabon, to meet some 50 children and young people living with or affected by HIV.
Accompanied by young Gabonese ambassadors for HIV and by artist Charly Tchatch, the animator of the opening of CAN 2017 and an AIDS activist, the international football star talked to the children and young people and listened to their stories and concerns. The children and young people talked about problems with accepting their status and stigma and depression, but also about happiness, love and how they deal with their daily problems.
“I am very touched. It is the first time I hear such poignant testimonies”, said Gervinho. “As you know, I wanted to play with my team here, but I am injured. Your mental strength and joy of life encourages me to face life’s challenges.” Gervinho signed the Protect the Goal campaign ball to support UNAIDS’ vision of zero new HIV infections, zero discrimination and zero AIDS-related deaths at CAN 2017.
Inge Tack, the UNAIDS Country Director, mentioned to Gervinho that despite AIDS budget cuts of 60% in Gabon since 2012, treatment rates have doubled and new HIV infections have been reduced by 30%, while paediatric treatment rates have tripled and coverage of prevention of mother-to-child transmission is at 78%. However, she also noted the need to improve the management of HIV treatment provision to achieve the 90–90–90 targets. “A radical shift in the organization and management of treatment delivery services is required to achieve the 90–90–90 targets in Gabon. Medicines need to be in the centre at all times and services reoriented to better serve patients’ needs,” said Ms Tack.
Gabon experiences persistent treatment stock-outs and poor care services result in no treatment adherence follow-up, no monitoring of drug resistance and no viral load measurement. Ms Tack stressed the need for a decentralized approach for the provision of antiretroviral therapy and an increase in community-led services.
Region/country
Related
Impact of the pause of US foreign assistance in Côte d'Ivoire
19 February 2025


Update
Training on age of consent manual piloted in Zimbabwe
09 December 2016
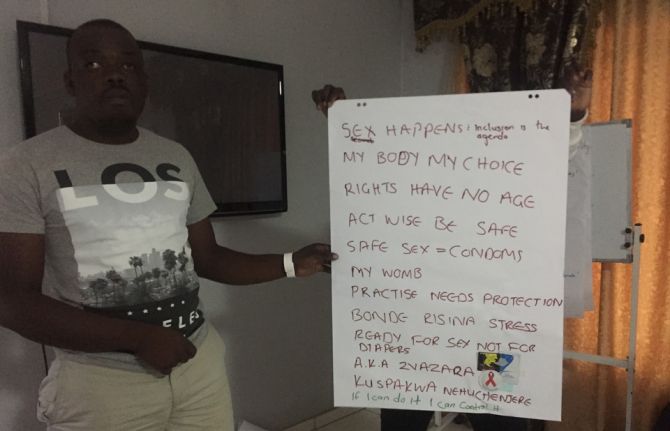
09 December 2016 09 December 2016“Age of consent: my body, my rights”, “Rights have no age” and “#Sex happens” were some of the creative advocacy messages that young people came up with during the pilot training on an age of consent advocacy manual that took place in Harare, Zimbabwe.
As part of the All In partnership to end adolescent AIDS, UNAIDS and the PACT, a global coalition of 25 youth-led and youth-serving organizations and networks working on HIV, developed a comprehensive advocacy manual on age of consent policies that relate to the sexual and reproductive health and rights of youth and adolescents. The manual seeks to provide youth advocates with the skills and information they need to respond to legal barriers, specifically age of consent laws and policies related to sex, HIV and sexual and reproductive health services.
As stated in the UNAIDS Prevention gap report, “In many settings, parental and other third-party consent requirements for access to HIV and sexual and reproductive health services remain an important barrier to their uptake. Adolescents often are reluctant to seek services that require the consent of a parent or guardian. Similarly, laws that restrict people’s access to health services—for example, by requiring third-party authorization for accessing sexual and reproductive health services or by criminalizing certain consensual sexual behaviours—exclude people from the health information and services they need”.
The piloting of the manual in Zimbabwe was facilitated by Youth Engage, a youth-led advocacy organization that brought together 25 youth advocates from diverse backgrounds.
Young people, with support from the National AIDS Council of Zimbabwe, are now mobilizing and preparing for a dialogue with parliamentarians to discuss the age of consent laws on marriage, sex and HIV testing in Zimbabwe and young people’s access to sexual and reproductive health services.
The manual will soon be piloted in India and will become a key resource for advocates to challenge legal and policy barriers that pose obstacles for young people’s access to HIV and sexual and reproductive health services all over the world.
Quotes
“We advocate to policy-makers because we want them to hear public opinion, and young people are the public opinion on this issue.”
“Through the activities and discussions around the impact of legal barriers on youth and adolescent health, young persons were able to freely explore the issue and craft ways in which age of consent issues could be tackled.”
“To generate demand for HIV and sexual and reproductive health and rights services, country programmes need to revise the current ineffective and inadequate laws and policies that exist and act as a barrier to young people’s access to services, such as age of consent laws.”
Resources
Region/country
Related
Zambia - an HIV response at a crossroads
24 February 2025
Status of HIV Programmes in Botswana
20 February 2025




Feature Story
Reaching young people in Namibia with sexual and reproductive health services
13 December 2016
13 December 2016 13 December 2016The Namibia Planned Parenthood Association clinic in Windhoek is decorated with colourful murals, its walls brightly painted with red ribbons. It has the feel of a welcoming classroom or youth club rather than a medical site. And that’s the idea, because this facility offers sexual and reproductive health services, including HIV testing and counselling, to adolescents and young people aged up to 25 years old.
The site is staffed by young peer-to-peer counsellors, such as 20-year-old Claudia Ndinundjene, who offers a friendly ear to the clinic’s users and advises them on what to expect from the testing process. She can also give them information on how to protect themselves from unintended pregnancy and HIV and other sexually transmitted infections.
“It’s important for young people to be advised by other young people,” says Ms Ndinunjene, “People need to be helped in a non-judgemental atmosphere that meets their needs—they shouldn’t be asked a lot of questions, but just get the help they need, and quickly.”
The clinic carries out about 200 rapid HIV tests a week. The results are back within 15 minutes. People who test negative are given condoms and advice on how to stay HIV-free. People who test positive are immediately referred to a neighbouring clinic to get access to antiretroviral medicine, which can keep them healthy.
One of the biggest challenges is to get young people to adhere to treatment, especially when long queues translate into long waits at other clinics, which may also be less oriented to the specific needs of young people. That’s why the Executive Director of the clinic, Bravo Linosi, would like to expand services.
“We would like to be able to offer treatment services to the young people who come here as well as HIV testing and counselling,” says Mr Linosi. “This would make a huge difference to young people’s lives, helping them remain healthy by staying on treatment and also helping Namibia to end the AIDS epidemic by 2030.”
The commodities used at the clinic are provided by the government, while funding and other support comes from a range of partners, including UNAIDS and the Global Fund to Fight AIDS, Tuberculosis and Malaria.
The clinic offers Wi-Fi, so that young people can carry on with their homework or simply stay in touch with their friends online while at the clinic. Mr Linosi has plans for pool nights or TV soccer nights to attract more young men to the clinic. In this way, he hopes that HIV testing can become a more routine part of young people’s lives, particularly young men, whose service uptake is currently poor.
The clinic still sees some older adults who have turned 25 but don’t want to go anywhere else, having been visiting the site for several years.
“People feel happy here and they keep coming back to the clinic because they feel safe—that’s why they don’t want to go anywhere else,” says Nelapewa Baumuller, a senior nurse at the clinic.
Region/country
Related
Zambia - an HIV response at a crossroads
24 February 2025
Status of HIV Programmes in Botswana
20 February 2025

Feature Story
HIV prevention among key populations
22 November 2016
22 November 2016 22 November 2016Since 2010, the annual global number of new HIV infections among adults (15 years and older) has remained static, at an estimated 1.9 million. Members of key populations, including sex workers, people who inject drugs, transgender people, prisoners and gay men and other men who have sex with men, and their sexual partners accounted for 45% of all new HIV infections in 2015.
In some countries and regions, infection rates among key populations are extremely high—HIV prevalence among sex workers varies between 50% and 70% in several countries in southern Africa. One study from Zimbabwe found HIV prevalence rates of 27% for male inmates, 39% for female inmates and 60% for sex workers, with 9.6% of these getting newly infected between 2009-2014. New infections among gay men and other men who have sex with men have been increasing in all regions in recent years. Across countries, key populations are between 10 and 50 times in greater risk of HIV infection compared to other adults.
Criminalization and stigmatization of same-sex relationships, sex work and drug possession and use, and discrimination, including in the health sector, are preventing key populations from accessing HIV prevention services. Effective government support and community-based and implemented HIV prevention and treatment programmes that provide tailored services for each group are currently too few and too small to result in a significant reduction in new infections.
In order to achieve the target of reducing new HIV infections among key populations by 75% by 2020, a large-scale increase of programmes and the creation of an enabling social and legal environment are needed.
We must reduce new HIV infections among key populations
The global number of new HIV infections among adults has remained static, at an estimated 1.9 million, since 2010, threatening further progress towards the end of the AIDS epidemic.
New HIV infections among gay men and other men who have sex with men are rising globally, and there has been no apparent reductions of new infections among sex workers, transgender people, people who use drugs or prisoners. Studies conducted in southern Africa have found HIV prevalence 10–20 times higher among sex workers than among adults in the general population, with rates of HIV infection reaching 50% of all sex workers tested, and HIV prevalence reaching 86% in one study in Zimbabwe. A synthesis of studies including more than 11 000 transgender people worldwide estimates HIV prevalence to be 19.1%.
Key populations remain among the most vulnerable to HIV. Analysis of the data available to UNAIDS suggests that more than 90% of new HIV infections in central Asia, Europe, North America, the Middle East and North Africa in 2014 were among people from key populations and their sexual partners, who accounted for 45% of new HIV infections worldwide in 2015.
Reinvigorating HIV prevention among key populations requires domestic and international investments to provide key populations with tools, such as condoms and lubricants, pre-exposure prophylaxis and sterile needles and syringes, and testing and treatment. However, the design and delivery of such HIV combination prevention services is often limited by a reluctance to invest in the health of key populations and to reach out to them.
In many countries, key populations are pushed to the fringes of society by stigma and the criminalization of same-sex relationships, drug use and sex work. Marginalization, including discrimination in the health sector, limits access to effective HIV services. There is an urgent need to ensure that key populations are fully included in AIDS responses and that services are made available to them.
Guidelines and tools have been developed for and with the participation of key populations in order to strengthen community empowerment and improve the delivery of combination prevention services by community-led civil society organizations, governments and development partners.
The available evidence shows that when services are made available within an environment free of stigma and discrimination and involving key population communities, new HIV infections have declined significantly. For example, street youth in St Petersburg had a 73% decrease in HIV seroprevalence from 2006 to 2012, primarily due to decreased initiation of injection drug use. This marked reduction in the HIV epidemic among street youth occurred after implementation of extensive support programs and socio-economic improvements.
The replication of such successes and the scale-up of combination prevention programmes in all cities and sites where key populations live and work, implemented by countries and community organization networks, will help prevention efforts get back on track to achieving the target of reducing new HIV infections by 75% by 2020.
Quotes
“WHAT MATTERS IS THE LACK OF INCLUSION AND WIDESPREAD DISCRIMINATION. IT IS CLEAR THAT WE CANNOT END THE AIDS EPIDEMIC WITHOUT TAKING CARE OF THE NEEDS OF KEY POPULATIONS.”
Hands up for #HIVprevention — World AIDS Day campaign
Related


Update
HIV prevention among key populations
21 November 2016
21 November 2016 21 November 2016Since 2010, the annual global number of new HIV infections among adults (15 years and older) has remained static, at an estimated 1.9 million. Members of key populations, including sex workers, people who inject drugs, transgender people, prisoners and gay men and other men who have sex with men, and their sexual partners accounted for 45% of all new HIV infections in 2015.
In some countries and regions, infection rates among key populations are extremely high—HIV prevalence among sex workers varies between 50% and 70% in several countries in southern Africa. One study from Zimbabwe found HIV prevalence rates of 27% for male inmates, 39% for female inmates and 60% for sex workers, with 9.6% of these getting newly infected between 2009-2014. New infections among gay men and other men who have sex with men have been increasing in all regions in recent years. Across countries, key populations are between 10 and 50 times in greater risk of HIV infection compared to other adults.
Criminalization and stigmatization of same-sex relationships, sex work and drug possession and use, and discrimination, including in the health sector, are preventing key populations from accessing HIV prevention services. Effective government support and community-based and implemented HIV prevention and treatment programmes that provide tailored services for each group are currently too few and too small to result in a significant reduction in new infections.
In order to achieve the target of reducing new HIV infections among key populations by 75% by 2020, a large-scale increase of programmes and the creation of an enabling social and legal environment are needed.
Hands up for #HIVprevention — World AIDS Day campaign
Related
Documents
Get on the Fast-Track — The life-cycle approach to HIV
21 November 2016
In this report, UNAIDS is announcing that 18.2 million people now have access to HIV treatment. The Fast-Track response is working. Increasing treatment coverage is reducing AIDS-related deaths among adults and children. But the life-cycle approach has to include more than just treatment. Tuberculosis (TB) remains among the commonest causes of illness and death among people living with HIV of all ages, causing about one third of AIDS-related deaths in 2015. These deaths could and should have been prevented. Download slide deck