Feature Story
UNAIDS Brazil and Grindr sign agreement to expand HIV prevention efforts and strengthen community-led responses
30 July 2026
30 July 2026 30 July 2026UNAIDS Brazil and Grindr have signed a cooperation agreement to expand access to HIV prevention and to bring health services closer to the populations most affected by HIV.
The agreement creates a framework for cooperation and the development of joint initiatives over the next two years, including expanding access to Pre-Exposure Prophylaxis (PrEP) and Post-Exposure Prophylaxis (PEP), reducing regional inequalities in access to health services, and strengthening community-led initiatives.
"Grindr reaches millions of LGBTQ+ people every day, while community-based organizations bring deep local knowledge, trusted relationships, and decades of experience serving their communities. As new prevention tools redefine what is possible, Grindr for Equality is committed to working hand in hand with partners such as UNAIDS Brazil, community leaders, researchers, healthcare professionals, funders, multilateral organizations, industry partners, and ministries of health to bridge the gap between awareness and uptake," said Mohan Sundararaj, Managing Director of Grindr for Equality.
The partnership recognizes that digital solutions can bring reliable information closer to the people who need it most. Through this agreement, Grindr will serve as an important channel for connecting app users to public HIV prevention, testing, and care services, while UNAIDS will provide technical support and evidence-based content to guide these efforts.
The partnership will support the development of inclusive digital campaigns with messages providing information on combination HIV prevention, including PrEP, PEP, condoms, regular HIV testing, and HIV treatment.
Another strategic pillar is the use of geolocation features within the platform to direct users to nearby public health services. This approach will help expand access to information about healthcare facilities, PrEP and PEP dispensing sites, and networks of care available in local communities.
"UNAIDS Brazil is pleased to sign this partnership agreement with Grindr, which is very present in the lives of young populations we serve. This platform can help locate health services and facilitate access to prevention information, and this will be our joint commitment. Each day people are more connected to digital environments that are essential to close the misinformation gap," says Andrea Boccardi Vidarte, UNAIDS Country Director in Brazil.
The signing of the MoU formalizes and expands a relationship built through previous collaborations between UNAIDS Brazil and Grindr. In September 2024, Grindr and UNAIDS joined forces to increase the participation of people living with HIV in the second edition of the Stigma Index survey. More recently, during Lady Gaga’s concert in Copacabana in 2025, in Rio de Janeiro, UNAIDS, Grindr, and the City of Rio de Janeiro developed a joint prevention initiative aimed at concert attendees.
UNAIDS Country Director in Brazil receives award for leadership and support to LGBTQIA+ communities
Andrea Boccardi Vidarte was among those honoured at the Grindr for Equality Awards, which took place during the AIDS20206 conference. These awards recognize leaders and organizations for their outstanding contributions to the global HIV response and to advancing the health and well-being of LGBTQIA+ communities.
During the Grindr for Equality Hosting, Ms Boccardi received the Systems Change Leadership Award which recognizes policymakers and institutional leaders who drive structural change to advance LGBTQIA+ rights, strengthen HIV prevention, and promote equitable access to healthcare.
Region/country



Press Release
Failing to tackle inequality puts countries in pandemic danger, new research shows
30 July 2026 30 July 2026Analysis in the New England Journal of Medicine – co-authored by experts including Nobel laureate Joseph Stiglitz, leading epidemiologist Professor Sir Michael Marmot, and Chairperson of the One Economy Foundation and former First Lady of Namibia Monica Geingos – finds economic inequality, not conventional preparedness, has been the clearest predictor of how countries fared against pandemics, upending traditional assumptions about what actions governments need to take for health security. The new research from the Global Council on Inequality, AIDS and Pandemics finds that while technical capacity remains necessary, it is not sufficient. To respond to and prepare for pandemics effectively, governments need to include efforts to address inequality.
Call for “Inequality-Informed Pandemic Preparedness and Response”
Conventional understandings of what countries need to do to be ready to face pandemics are incomplete and need to be re-thought, the research shows. Many of the countries that score highest on standard measures of pandemic preparedness—based on technical abilities like laboratory, supply chain, or emergency response capabilities—have seen some of the highest rates of infection and death during both the COVID-19 and AIDS pandemics. Countries like the United States or United Kingdom have topped official preparedness lists, but the research findings show no association between these traditional understandings of preparedness and success in the real world. Policies that only ensure technical capability are not enough.
Inequality, on the other hand, is the clearest predictor of how a country fares when a pandemic strikes, with more unequal countries less successfully responding than their more equitable peers.
The research shows that the prevailing conception of pandemic preparedness as synonymous with technical capacities leads governments give too little attention to addressing the sources of inequality that shape the use of those capacities. The analysis demonstrates how proven, practical approaches can enable countries to overcome the inequalities which undermine public health. This includes addressing the social determinants of health within countries—the unequal conditions in which people are born, grow, live, work and age—as well as between-country inequalities in the global financial system. Countries could be mounting inequality-informed pandemic preparedness and response today – but they are not.
Four ways governments can break the cycle
The research sets out proven, practical and affordable policies to address the inequalities driving pandemic risk, so that countries can respond more effectively to HIV, tuberculosis, Ebola and other pandemics. The actions governments need to take include:
- Protecting people during outbreaks: surge social protection such as paid sick leave, cash transfers and unemployment support, so no one has to choose between following health advice and feeding their family – alongside long-term investment in housing, education and secure work to build resilience before the next crisis.
- Governing across society, not health alone: multi-sectoral planning that brings in finance, labour and education ministries, and embeds community-led organisations in the response, drawing on hard-won lessons from the AIDS pandemic.
- Fixing the global financial rules: a debt-standstill mechanism for countries facing emergencies, the automatic release of emergency international financing when a pandemic is declared, and expanded pandemic lending so that every country has the means to respond.
- Sharing life-saving science: open licensing of publicly funded research, a global prize fund that rewards innovators while allowing medicines and vaccines to be produced anywhere, and expanded regional manufacturing of the treatments and vaccines needed to stop today’s and tomorrow’s pandemics.
Expert call
The analysis and call to action is outlined in the latest edition of the New England Journal of Medicine by Nobel Laureate Joseph Stiglitz, leading epidemiologist Sir Michael Marmot, Chairperson of the One Economy Foundation and former First Lady of Namibia Monica Geingos, UNAIDS Executive Director Winnie Byanyima, and incoming Chair of the Department of Global Health and Director of the Center for Global Health Policy & Politics at Georgetown University Matthew Kavanagh. The New England Journal of Medicine article, “The Inequality–Pandemic Cycle — Rethinking Preparedness”, setting out the argument and the way forward, is available here, and the accompanying full background data analysis can be read here. They are part of an ongoing programme of research by the Global Council on Inequality, AIDS and Pandemics, an international, interdisciplinary expert group convened by UNAIDS.
“For decades the world judged how ready a country is for a pandemic by counting its laboratories, stockpiles and response plans,” said Joseph Stiglitz, Nobel Laureate in Economics and Co-Chair of the Global Council. “This research shows that this is not enough. High economic inequality can leave even wealthy, well-equipped nations dangerously exposed. The encouraging news is that inequality is not inevitable – it is the result of policy choices, and we know how to change them. Reducing inequality is now one of the smartest investments any government can make.”
“Inequality is the ground in which pandemics take root – and this research proves it,” said Winnie Byanyima, Executive Director of UNAIDS, which convenes the Global Council. “It also shows leaders exactly where to act. By tackling the inequalities within our societies, we can end AIDS as a public health threat and make the world safer from the next pandemic. When we address inequality, everyone thrives.”
The research is being published just ahead of a special panel discussion taking place at AIDS 2026 in Rio de Janeiro – the biennial gathering of the leaders of the international HIV response. The panel, at 10:30am Rio time on 30th July, will include Joseph Stiglitz, Winnie Byanyima and Matthew Kavanagh alongside Nísia Trindade, Former Minister of Health of Brazil, Javier Padilla Bernáldez, Secretary of State for Health of Spain, and Richard Lusimbo, Director General of The Uganda Key Populations Consortium.
Pandemic emergency
The AIDS pandemic, the largest disease of the last century, has killed at least 44 million people globally since the early 1980s. Approximately 40.8 million people are living with HIV globally, while over 9 million are not on treatment because of inequalities obstructing access, putting them at risk of dying of AIDS-related illnesses. COVID-19 and AIDS have caused far more deaths combined than all the wars over the last half-century.
The new analysis tested why some countries have more effectively tackled COVID-19 and AIDS than others. It found that a country’s level of economic inequality consistently predicted death and infection rates – while conventional preparedness rankings and levels of poverty did not. Some of the countries rated most prepared before COVID-19, including the United States, went on to record death rates far above the global average, while lower-ranked countries such as Vietnam and Ethiopia fared far better. The reason, the researchers set out, is that inequality shapes whether a country can actually mobilise the tools it has: who can afford to stay at home, who trusts public institutions, and who is reached by health services. This makes tackling inequality an essential part of enabling true preparedness.
There is a clear and consistent association between inequality and less effective response. The numbers are stark. Using the Gini coefficient – the standard 0–100 measure of income inequality – the researchers found that every one-point rise in a country’s inequality was associated with around 12.5 additional COVID-19 deaths for every 100,000 people. This pattern held for AIDS deaths and new infections as well. The pattern held across the countries studied and remained just as strong when poverty and conventional measures of preparedness were taken into account.
Economic inequalities intersect with other social determinants of health. Key populations, including men who have sex with men, transgender people, sex workers, people who inject drugs, and incarcerated people, face barriers in accessing vital services, exacerbating their risk of HIV infection. Girls in Africa face higher risk of HIV than boys. These inequalities are not inevitable and can be overcome through effective public policies.
Inequality and pandemics reinforce one another. Inequality leaves societies more exposed when outbreaks hit, and pandemics in turn widen existing gaps both within and between countries, deepening the very conditions that make future outbreaks harder to control. An International Monetary Fund analysis of past outbreaks found income inequality kept rising for around five years after each one. Breaking this cycle, the authors argue, is now essential to global health security.
As the world confronts multiple pandemics and the rising risk of new ones, the Global Council is calling on world leaders to place inequality at the centre of pandemic preparedness and response to avert another crisis of COVID-19 proportions or worse. More than 90% of the global population now lives in a country with high income inequality – levels not seen since the industrial revolution – leaving the world more exposed than ever.
“Health is not distributed by chance – it follows the conditions in which people are born, grow, live, work, and age, and those conditions are deeply unequal,” said Professor Sir Michael Marmot, Director of the UCL Institute of Health Equity and Co-Chair of the Global Council. “The inequalities that damage health in ordinary times are the same ones that leave whole societies exposed when a pandemic strikes. Creating fairer conditions of daily life is not a nice-to-have – it is the foundation of health security.”
“The evidence is clear: out-of-control inequality is bad for everyone’s health. Effective pandemic preparedness includes taking practical action to tackle the inequalities which drive them,” said Monica Geingos, Chairperson of the One Economy Foundation, former First Lady of Namibia, and Co-Chair of the Global Council.
“This is about political choices,” said Matthew Kavanagh, incoming Chair of the Department of Global Health and Director of the Center for Global Health Policy & Politics at Georgetown University, and Member of the Global Council. “Investing in tackling inequality will keep people safe.”
UNAIDS
The Joint United Nations Programme on HIV/AIDS (UNAIDS) leads and inspires the world to achieve its shared vision of zero new HIV infections, zero discrimination and zero AIDS-related deaths. UNAIDS unites the efforts of 11 UN organizations—UNHCR, UNICEF, WFP, UNDP, UNFPA, UNODC, UN Women, ILO, UNESCO, WHO and the World Bank—and works closely with global and national partners towards ending the AIDS epidemic by 2030 as part of the Sustainable Development Goals. Learn more at unaids.org and connect with us on Facebook, Twitter, Instagram and YouTube.
Contact
Oliver Aplintel. +44 7851552441
oca10@georgetown.edu
Ben Phillips
tel. +66 613649866
ben.phillips@globalcooperation.institute
At AIDS 2026 in Rio
Daniel De Castro
tel. +507 69983175
DeCastroD@unaids.org
Robert Shivambu
tel. +27 836081498
shivambuh@unaids.org
Documents
Opening remarks at AIDS2026
28 July 2026
So my message is simple. We must build something new—an AIDS response for the world that we have today, not the world we wish existed. Not the world of yesterday.

Documents
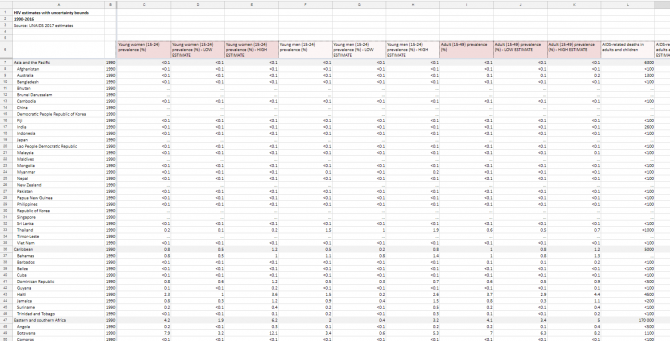
HIV estimates with uncertainty bounds 1990-2025
27 July 2026
HIV estimates with uncertainty bounds 1990-Present. Download spreadsheet Updated 27 July 2026.
Documents
Methods for deriving UNAIDS HIV estimates
27 July 2026
Documents
Special report AIDS2026 slides
27 July 2026
Documents
UNAIDS Special Report for the 26th International AIDS Conference
27 July 2026
Data collected by the Joint United Nations Programme on HIV/AIDS (UNAIDS) from countries show that HIV funding disruptions severely impacted HIV prevention, testing and key components of treatment programmes, such as the range of community-led services that reach the people most affected by HIV. These funding shifts prompted countries to prioritize short-term domestic resource mobilization to preserve essential HIV treatment services—a necessary first step in sustaining national HIV responses. The full effects of the funding cuts on the global HIV response will become evident over the next few years as HIV programmes re-emerge with new sources of funding.
Related materials:
Press Release
Global HIV response falters as reemergence looms
27 July 2026 27 July 2026In 2025, 1.2 million more people became infected with HIV and 570 000 more people died of AIDS-related illnesses as the world fell short of global targets. Without urgent action to meet the 2030 goals, more than 3 million could become infected with HIV by 2030.
RIO DE JANEIRO/GENEVA, 27 July 2026—A special report released by UNAIDS for the 26th International AIDS Conference taking place in Rio de Janeiro, Brazil from 27 to 31 July, shows that reductions to international funding and cuts to HIV prevention and community services are likely to lead to a resurgence of the epidemic.
Although new HIV infections and AIDS-related deaths are at their lowest levels in more than 30 years, the current HIV response is extremely fragile. Efforts to end AIDS as a public health threat by 2030 are at risk unless global solidarity is restored and inequalities are addressed.
In 2025, 1.2 million people acquired HIV, but progress is uneven. New HIV infections rose in three regions and 21 countries in 2025. Around 9 million of the 41 million people living with HIV were not on treatment and almost half of all children living with HIV did not have access to antiretroviral therapy in 2025. More than half a million people (570 000) died of AIDS-related illnesses in 2025.
Positively seven countries* achieved an almost 80% reduction in new infections since 2010 and 11 countries achieved the 95-95-95** treatment targets showing that progress is possible.
Science and innovation offer a major opportunity. The world is on the cusp of an HIV prevention revolution in prevention medicines which offer close to vaccine like protection against HIV. Monthly and six-monthly injections are slowly trickling into the market, and monthly pills are in late-stage trials. What is coming to market and in the pipeline is extraordinary, however the challenge remains scale and inequitable access.
“Scientific breakthroughs are giving us tools that previous generations could only dream of,” said Ms Byanyima. “However, innovation without access is not innovation, it is injustice. The test of success is not whether medicines exist—it is whether the people who need them can get them, and at an affordable price.”
Brazil has increased the number of people accessing HIV prevention medicines at least once in the past year by 41%. Ethiopia and Uganda also took action to expand access through domestic and other funding, and South Africa is continuing to negotiate pricing deals for the twice-yearly prevention injections lenacapavir. However, despite being part of the trials for lenacapavir, Brazil has not been granted voluntary licensing from producer Gilead to enable cost-effective pricing or the introduction of generic alternatives and is considering compulsory licensing.
UNITAID, the Global Fund to Fight AIDS, TB and Malaria and partners have pulled money together to start rolling out lenacapavir to reach 3 million 2028 which is welcome news, but this remains a drop in the ocean, currently reaching just a few thousand people. UNAIDS estimates that 20 million people need of access to antiretroviral based prevention to have a real impact in stopping new HIV infections.
Overseas development assistance (ODA) has collapsed. Global development assistance from multiple countries fell by 23% in 2025—the sharpest drop on record—a large proportion of which was for global health and HIV programmes have been hit hard.
High burden, highly indebted, low-income countries of Africa depended on ODA for the success of their AIDS responses. Many of these countries were more than 90% dependent on ODA for their HIV responses.
“The era of relying on international aid is over,” said Winnie Byanyima, Executive Director of UNAIDS. “Countries cannot wait and they cannot go backwards. The world must urgently fix the broken financial system and accelerate debt restructuring so that governments can invest in what matters most—the health, education and futures of their people.”
International financing for HIV from multiple countries declined by more than US$ 1.5 billion, from US$ 8.8 billion in 2024 to US$ 7.3 billion in 2025, an 18% reduction and the lowest level in nearly two decades.
HIV prevention services were largely funded from international funding. For example, in sub-Saharan Africa, 80% of prevention funding came from international aid. Community-led organizations received up to 25% of foreign HIV assistance in 2024. Surveys show that in some countries these organizations reached 22% of people living with HIV and up to 60% of marginalized populations with life-saving services. With the absence of donor support and stronger domestic investment, HIV prevention and community-led HIV service delivery risk total collapse.
Funding for condoms has been cut by more than 90% in some countries. A 2026 study, across 47 countries, found steep reductions in community-led services—50% for community-led support for prevention medicines and HIV care—85% for services for gay men and other men who have sex with men—82% for sex workers—and 72% for survivors of gender-based violence.
Human rights are under attack and there is a reversal of rights including the sexual and reproductive rights of women and girls and marginalized populations. For the first time since UNAIDS has been tracking these trends, criminalization of marginalized populations increased. In 2025, Burkina Faso and Niger introduced criminalization of same-sex sexual activity, and Senegal increased penalties for same-sex sexual activity in 2026.
In 2026, 168 countries criminalized sex work, 152 countries criminalized possession of small amounts of drugs, 66 countries criminalized same sex sexual relations, and 14 countries criminalized transgender people.
“You cannot end AIDS while criminalizing people living with and most at risk of HIV,” said Ms Byanyima. “When people fear arrest, violence or discrimination, they stay away from HIV services. Human rights are not separate from the HIV response—they are essential to its success.”
Despite the push back on human rights, in June 2026, 149 Member States adopted a progressive Political Declaration on HIV and AIDS aligned with the UNAIDS Global AIDS Strategy 2026–2031 and its 2030 targets. The new 2030 targets include 40 million people on life-saving treatment, 20 million with access to antiretroviral-based prevention. The targets also include less than 10% of people living with or at risk of HIV experiencing stigma and discrimination, less than 10% of women and girls and people living with or at risk of HIV experiencing gender inequality and violence, and less than 10% of countries having punitive legal and policy environments that deny or limit access to HIV services. If fully achieved, the commitments would avert an additional 3.2 million new HIV infections and 1.3 million AIDS-related deaths by 2030.
“Despite enormous challenges ending AIDS is still within reach,” said Ms Byanyima. “At AIDS 2026 UNAIDS is urging all partners and governments to remobilize and push forward to achieve the ambitious targets in the Political Declaration. This will require renewed solidarity, sustained financing and unwavering commitment to human rights. The choice before us is clear: retreat and risk resurgence, or rethink, rebuild and rise to end AIDS as a public health threat by 2030.”
*Benin, Eswatini, Kenya, Lesotho, Nepal, Rwanda and Zimbabwe
**95% of all people living with HIV who know their status, 95% of all people with diagnosed HIV infection accessing antiretroviral therapy, 95% of all people accessing ART who are virally suppressed.
UNAIDS
The Joint United Nations Programme on HIV/AIDS (UNAIDS) leads and inspires the world to achieve its shared vision of zero new HIV infections, zero discrimination and zero AIDS-related deaths. UNAIDS unites the efforts of 11 UN organizations—UNHCR, UNICEF, WFP, UNDP, UNFPA, UNODC, UN Women, ILO, UNESCO, WHO and the World Bank—and works closely with global and national partners towards ending the AIDS epidemic by 2030 as part of the Sustainable Development Goals. Learn more at unaids.org and connect with us on Facebook, Twitter, Instagram and YouTube.
Documents
UNAIDS Executive Director's remarks at the Extraordinary Session of the African Union Assembly on Ending AIDS by 2030
24 July 2026


Feature Story
"Funding Community-led harm reduction is not optional to end AIDS” - An interview with Anton Basenko
23 July 2026
23 July 2026 23 July 2026UNAIDS sat down with Anton Basenko, Executive Director of International Network for People who Use Drugs (INPUD) during the latest coordinating board meeting where Member States and partners discussed how people who inject drugs are disproportionately impacted by the HIV epidemic worldwide.
In 2024, HIV prevalence among people who inject drugs reported was ten times higher than for the rest of the adult (15–49 years) population and people who inject drugs were estimated to be 34 times more likely to contract HIV than the general adult population.
Q: How did you become an activist and advocate?
A: I began using drugs as a teenager and started injecting when I was 16. Like millions of people around the world, I spent years avoiding healthcare not because I did not need it, but because healthcare did not feel safe.
In 2002, Ukraine started to scale up the limited offer of harm reduction services. I did not go there because someone convinced me to seek treatment. I went to a drop-in centre run by Club Eney because I needed sterile injecting equipment. What I found there was much more than syringes. After almost 10 years of spending days looking for money, avoiding the police and buying drugs, I was in awe of the peer-led, peer-run place and realized, 'People care about me.'
I had lost many friends and suffered many overdoses and lost my job so this outreach was like a miracle. That is where later, in 2023, I found out I was HIV+ and had Hepatitis C and needed treatment. I also qualified for opioid agonist therapy (OAT), which is another miracle. They were running a pilot programme at the time. Within months I transformed and regained confidence. So much so that when it was time to validate the pilot programme, I was asked to testify at the Ministry of Health Public Hearings. Wearing a tie and speaking about my experience, I overheard people from the opponents of the OAT group say afterwards, 'His outfit is too expensive and he looks too clean to be a real drug user,' which made me think that OAT definitely works and I clearly had convinced people from all sides during the meeting.
Q: When is it that you really pushed for harm reduction services?
A: In 2005, I went to the OAT site at the Kyiv Narcological Dispensary to get my daily dose of medicine and saw that the door was closed. I was in total shock and I felt all my hopes disappear. The majority of us were so afraid of withdrawal symptoms that we relapsed. Ukraine was in the midst of rolling out harm reduction and there had been a backlog. I was an emotional train wreck. Thank goodness the centre called us back a month and half later and I was able to get back on the medicine. It took me six months to get back on track. That experience taught me that policies are not written in isolation. They determine whether people live or die. They determine whether services remain open or disappear. And they determine whether communities are treated as partners—or as problems. Today, more than twenty years later, that lesson remains just as relevant.
Q: Was that a turning point for you?
A: It definitely motivated me and as of 2009 I volunteered and started working for a grassroots organisation in Kyiv as a peer-counselor at the OAT site. Slowly I left my marketing job and dedicated myself to the cause. At first, I worked for the Association of Substitution Therapy Advocates of Ukraine (ASTAU), and later joined the leading HIV CSO in EECA region, Alliance for Public Health. Feeling my commitment to invest my knowledge and motivation into the development of the global drug users’ rights movement and communities mobilisation, I co-founded Ukrainian Network of People who Use Drugs (VOLNa), contributed to the Eastern European Central Asian Network of People who Use Drugs (ENPUD), and worked for European AIDS Treatment Group (EATG.) I have also given a lot of speeches at AIDS and Harm Reduction conferences! And after being on the board of INPUD, I was appointed as INPUD Executive Director in 2025.
Q: INPUD's latest report ' The Human Costs of Policy Change: A World in Turmoil' documents the impact of recent funding cuts. What are they?
A: We are witnessing needle and syringe programs closing or being severely reduced. A lack of access to harm reduction supplies spiked from 47% in 2025 to 64% in 2026, stigma and discrimination jumped from 60% to 77%, policing or criminalisation increased from 42% to 64%. For women who use drugs, the consequences have been even more severe, with reductions in gender-based violence services, child-friendly spaces and low-threshold treatment programs. As someone who has lived through HIV, hepatitis C, criminalisation and exclusion from healthcare, I know that people do not stop using drugs because services disappear. They simply disappear from services until they return with advanced HIV, tuberculosis, hepatitis C, or... they DO not return at all.
Q: What is your main call to action?
A: The lesson is clear. Funding community-led harm reduction is not optional. It is one of the most cost-effective investments in the HIV response. We cannot end AIDS while allowing the organisations closest to affected communities to disappear. INPUD wants donors, partners, governments to protect and expand sustainable, direct and flexible funding for community-led organisations of people who use drugs and safeguard comprehensive harm reduction services, including needle and syringe programmes and opioid agonist therapy. Also know that the funding cuts collided with criminalisation and shrinking civic space which has been horrible. We must accelerate drug policy reform, including decriminalisation, as an essential structural intervention to end AIDS.
Q: You keep hammering one message, what is it?
A: Our message is simple: if communities disappear, the HIV response disappears with them.
Q: And what are you proudest of?
A: Professionally, I am very happy to have started harm reduction programmes in probation services. It has gone from a pilot programme to full scale in Ukraine and proud to mobilise the successful country drug users network, VOLNa, which unites more than 1,500 individual members and is a real driver of critical changes in Ukraine and EECA region.
I am also very proud of my son who is now seven years old living free of HIV.
UNAIDS advocates for harm reduction responses to be tailored to the realities of people who use drugs, recognizing that HIV risk and access are shaped by gender inequality, age, sexual orientation, incarceration, displacement and humanitarian crises. We must move away from criminal sanctions for drug use and possession for personal use and instead adopt public health and human-rights based approaches. Integrating harm reduction into national health systems and domestic financing frameworks will guarantee that essential services do not stop putting people’s lives at risk. Finally, UNAIDS believes in strengthening and protecting community leadership. Organizations led by people who use drugs must be able to register, operate and access funding freely.